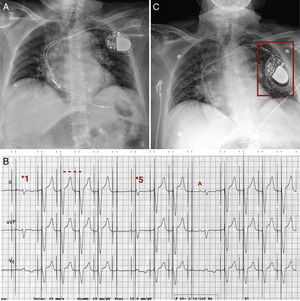
The electrocardiogram (Figure, panel B) shows the double spikes typical of dual-chamber (DDD) pacemakers. The first beat (*1) corresponds to the native QRS following the double spikes, with a prolonged PR interval, indicating the loss of ventricular capture. This loss is not permanent; the following 4 beats show a paced QRS (----) and the fifth (*5), again a loss of capture. The P waves are evident (^), but there are no adequate data on atrial detection or capture.

The diagnosis is reel syndrome (option 3), caused by lead dislodgement due to generator rotation over its sagittal axis.1 The lead winds around the generator as though the latter were a reel (Figure, panels A and C) (Figure, panels A and C: chest radiographs following implantation and in the emergency department, respectively). In twiddler syndrome, the rotation of the generator causes the lead to wind around itself, forming a braid.1 In ratchet syndrome, there is no rotation and, usually, only the lead is affected.1 Option 4 is a distractor; the dislodged atrial lead can be seen in the generator pocket (Figure, panel C), and caused the spasms in the upper extremity described by the patient.