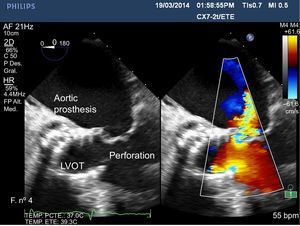
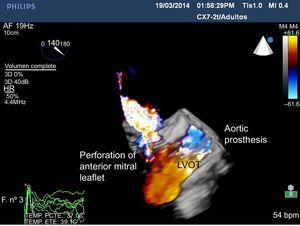
An 86-year-old male patient with percutaneous implantation of a CoreValve self-expanding aortic valve suffered complete atrioventricular block, which was treated with implantation of a permanent pacemaker. One week later, he was seen at the Emergency Department for fever, general malaise, and pain in the pacemaker pocket, with signs of sepsis. Antibiotic treatment was started and we decided to remove the pacemaker; the patient later showed symptoms suggestive of cerebral stroke (right hemiplegia and dysarthria) due to a parieto-occipital intraparenchymal hematoma and a blood culture that tested positive for Staphylococcus aureus. As endocarditis of the aortic valve was suspected, we performed a 2-dimensional (Figure 1) and 3-dimensional (Figure 2) transesophageal echocardiography of the left ventricular outflow tract (LVOT), showing mild aortic regurgitation with no increased gradients in the prosthesis and moderate mitral regurgitation due to perforation of the anterior leaflet caused by the prosthetic stent; no vegetation or perivalvular abscesses were observed. Despite antibiotic treatment and removal of the pacemaker, the patient died a few days later.


In this patient, the valve's self-expanding stent perforated the anterior mitral leaflet. Together with the infection in the pacemaker pocket, this favored the onset of endocarditis in that location, complicated by septic brain embolism.
Anterior mitral leaflet perforation is a rare complication following percutaneous implantation of an aortic valve, for which treatment is not well established. Replacing both valves is a possibility, but is not always feasible in patients with high surgical risk.