Ebstein's anomaly accounts for 0.5% of all congenital heart diseases. The condition is characterized by >8 mm/m2 displacement of the septal and posterobasal tricuspid leaflets toward the apex of the right ventricle (RV). This causes "atrialization" of the RV inflow tract, with decreased size of the RV and right atrial (RA) dilatation. The anterior valve is rarely displaced, but tends to be large and redundant. Associated tricuspid regurgitation (TR) and atrial shunt are common.
Fetal echocardiography allows the diagnosis of Ebstein disease and is an aid to planning management of the condition during gestation and after birth. Pulmonary hypoplasia, severe TR, and pericardial effusion are signs of a poor prognosis.
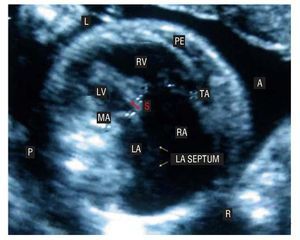
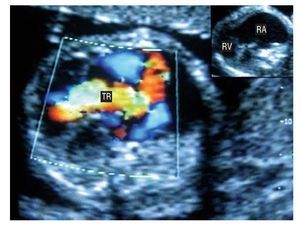
We present the case of a 21-week-gestation fetus referred for atrial dilatation. Fetal echocardiography showed a horizontally oriented heart, severe cardiomegaly with right cavity predominance, and considerable RA dilatation. A pronounced, 4.6-mm separation (S) was seen between the tricuspid and mitral valves. The mitral annulus (MA) and tricuspid annulus (TA) measured 0.79 and 1.74 cm, respectively (Figure 1). The imaging findings included severe TR reaching the RA roof, with a 6-mm jet at the origin (Figure 2) that caused a severe pulmonary functional obstruction. In addition, pulmonary artery hypoplasia and anterior pericardial perfusion (PE) of 3 mm were evident.

Figure 1.

Figure 2.
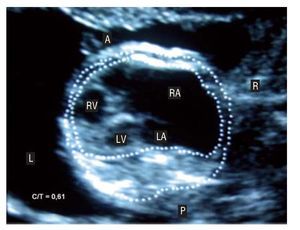
The fetus was severely affected, with signs of congestive heart failure, severe cardiomegaly (cardiothoracic index [C/T] = 0.61) (Figure 3), pericardial effusion, and pulmonary hypoplasia. This type of presentation is associated with elevated intrauterine mortality.

Figure 3.