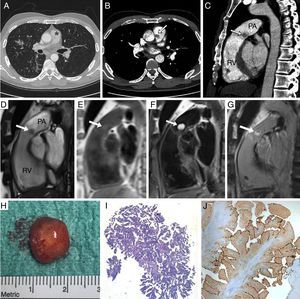
A 45-year-old man with Crohn disease was referred for colectomy. Preoperative chest X-ray showed a right pulmonary hilum nodular image that prompted a thoracic computed tomography scan. Incidentally, a round mass was detected in the main pulmonary artery (Figure A, asterisk) and was further confirmed on computed tomography-angiography (Figure B-C; arrows; PA, pulmonary artery; RV, right ventricle). The patient denied prior chest pain, palpitations, dyspnea, or fever. Transthoracic and transesophageal echocardiography identified a round mass attached to the arterial side of the pulmonary valve, with no valve regurgitation. A magnetic resonance scan confirmed the presence of a 12-mm diameter mobile mass attached to the pulmonary valve, which was isointense on T1-weighted images, highly hyperintense on T2, and was not perfused but was enhanced 10minutes after gadolinium administration (Figure D-G, arrows; Video 1 of the supplementary material). Thus, the differential diagnosis between pulmonary valve papillary fibroelastoma and myxoma was established. Cardiac surgery was performed 1 month after colectomy. A well-defined round mucinous mass attached to the tip of the pulmonary valve was easily excised, with valve sparing (Figure H; Video 2 of the supplementary material). It consisted of an elongated and branching papillary proliferation covered by a single layer of cells (Figure I) on hematoxylin-eosin stain, which expressed endothelial cell markers (Figure J) on immunohistochemistry for erythroblast transformation-related gene, thus allowing diagnosis of papillary fibroelastoma.

Papillary fibroelastomas are common, but not in a pulmonary position. The differential diagnosis with myxoma can be difficult, mainly if the masses are round-shaped. Magnetic resonance findings facilitate the diagnosis of a wide range of masses.