To the Editor:
Left anterior congenital diaphragmatic hernia is a highly uncommon defect. In adults, its diagnosis is generally incidental, whereas in children, it frequently produces signs of respiratory disease.
A 13-month-old boy, previously diagnosed as having a small ostium secundum atrial septal defect, was referred to our center to be studied because of poor echocardiographic visualization. The mother denied having any type of cardiorespiratory symptoms. The personal history of the infant included a postnatal diagnosis of Down's syndrome (mosaicism) and congenital hypothyroidism, with hormone replacement therapy. He was in good general health, afebrile, and eupneic. Chest auscultation revealed rhythmic, although slightly muffled, heart sounds, in the absence of murmurs, and mild hypoventilation at the base of left hemithorax, with bowel sounds at that level. The echocardiographic study (Figure 1) showed anterior basal pericardial effusion of up to 17 mm during diastole, with no evidence of hemodynamic impact. The cardiac structures were displaced to the right, but had a normal configuration; it was not possible to obtain parasternal views. Plain chest x-ray (Figure 2) revealed the presence of air in left hemithorax that obscured the cardiac border, suggestive of anterior diaphragmatic hernia, which was confirmed by means of ultrasound and magnetic resonance imaging of chest and abdomen. Oral treatment with acetylsalicylic acid (100 mg/kg body weight/day) and methylprednisolone (an initial bolus of 2 mg/kg and 2 mg/kg/day thereafter) was initiated and was maintained for 1 week, resulting in a considerable improvement in the effusion (8 mm after 48 hours). The studies performed included differential blood cell count, blood chemistry, thyroid hormones, antinuclear antibodies, rheumatoid factor, Mantoux test, and serological testing for Echovirus, Coxsackievirus A and B, adenovirus, Influenza, Varicella, Epstein-Barr, and human immunodeficiency virus, with normal findings in every case. The effusion remained stable, and surgical repair of the hernia was carried out by means of laparotomy 3 weeks after the diagnosis, with very good results. There has been a progressive reduction of effusion (3 mm 6 months after surgical intervention).

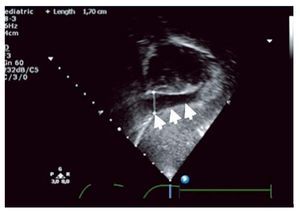
Figure 1. Echocardiography (subcostal view). Moderate anterior basal pericardial effusion.

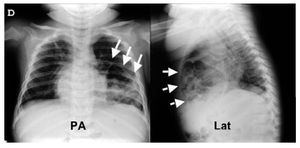
Figure 2. Chest x-ray. The posteroanterior projection (PA) demonstrates the presence of air obscuring the internal cardiac border and linear limit at its apex. The lateral projection (Lat) confirms the basically anterior position, with images of air that present portions of the intestine in their interior.
Congenital diaphragmatic hernia is an uncommon lesion (estimated prevalence, 1/2000 to 1/5000 live births). Morgagni hernia (anteriorly located) represents 3% to 5% of all of these hernias, and there is a clear predominance of the right parasternal position (at a ratio of 10:1), as the left side is protected by the pericardium.1
Thus, the incidence of the lesion we describe (left anterior congenital diaphragmatic hernia or Morgnani-Larrey hernia) is exceptionally low. Although cases have been reported in fetuses and newborn infants, it is generally produced as a consequence of acquired mechanisms that increase the intraabdominal pressure, resulting in herniation of the abdominal organs into the thoracic cavity through a congenital anatomical defect in the left sternocostal triangle of the diaphragm. In adults, it usually goes undetected and the diagnosis is incidental, whereas in children, it frequently produces respiratory symptoms (dyspnea, tachypnea, and recurrent pneumonia).1,2 Cases have been reported of newborn infants with associated severe pericardial effusion, often treated by means of emergency pericardiocentesis followed by corrective surgery. However, the slow development of the effusion due to the direct irritation of the pericardial sac can result in the accumulation of a significant amount of fluid with no hemodynamic impact. Thus, it would appear to be reasonable to adopt an initial conservative approach and perform definitive surgical treatment electively.3 In our case, we decided to initiate medical treatment in order to reduce the effusion, which proved to be effective, and subsequent elective surgery. Initially, we suspected a thyroid hormone deficiency (a disorder associated with trisomy 21) as a possible cause, despite the fact that a complete etiological study was carried out and all the results were negative. Since an association between Morgagni hernia and trisomy 21, although not very common, has been demonstrated, the former should be considered in the presence of recurrent respiratory and/or gastrointestinal conditions or those of unknown cause in patients with chromosomal abnormality.4,5
In a case of Morgagni-Larrey hernia as an unusual cause of pericardial effusion in a child with Down's syndrome, the slow and progressive development of the effusion makes it possible, in many cases, to adopt an initial conservative approach, to be followed subsequently by definitive surgery performed electively.