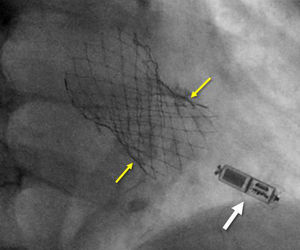
An 87-year-old man underwent transcatheter aortic valve implantation (TAVI) (CoreValve, Evolut, No.° 34) to treat severe aortic valve stenosis with symptoms of dyspnea. He was receiving chronic acenocoumarol therapy due to a history of pulmonary thromboembolism and had not experienced episodes of syncope. The preprocedure electrocardiogram showed sinus rhythm, a PR interval of 235ms, and a left anterior fascicular hemiblock. Following implantation, which was somewhat deeper than planned (at 10mm from the aortic valve annulus [Figure, yellow arrows]), moderate aortic insufficiency was observed. Postdilatation with a 25mm balloon was then performed and the degree of aortic insufficiency decreased to mild on both angiography and transesophageal echocardiography. Although there was no evidence of a new electrocardiographic abnormality, a temporary pacemaker was placed and the patient was started on dual antiplatelet therapy. During his stay in the coronary unit, the patient had runs of complete atrioventricular block. Because of his frailty and to decrease the risk of bleeding, we decided to implant a leadless pacemaker (Micra, MC1VR01 [Figure, white arrow]). The procedure was performed the next day using a right femoral approach, with device implantation in the right ventricle at the interventricular septum. The pacing parameters were excellent and the patient had a favorable clinical course without complications.

The excellent outcome of our patient following TAVI and Micra placement suggests that this combined therapy could be an attractive option to reduce bleeding complications and decrease length of hospitalization in selected patients.