To the Editor:
A 26-year-old woman, with no relevant personal or family history, experienced 3 resting syncopal episodes with tonic convulsions in a period of 2 months. The physical examination, electrocardiogram, echocardiogram, programmed stimulation, and a provocation test with flecainide were normal or negative. A subcutaneous Holter was implanted (Reveal® Plus Medtronic, Inc.) which was consulted a fortnight later after a new syncope with the same features. Ventricular fibrillation (VF) was substantiated (Figure, A) initiated by a ventricular extrasystole (VE) (Figure, B, arrows). In the minute prior to the event, a large density of VE from the same focus with fixed coupling (Figures, A and B). The VF was maintained for almost 3 minutes and spontaneously ceased (Figure, C), the VE disappeared in the following minutes (Figure, A). An ablation of the VE was attempted which set off the VF, but its reproduction was not possible during the electrophysiological study. The implanting of a defibrillator was decided on. Two months later, the patient underwent treatment with beta blockers and no clinical events were registered.

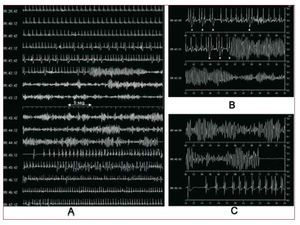
Figure 1. A: complete register of the ventricular fibrillation with the Holter insert; 1 minute before the appearance of a large density of ventricular extrasystoles which disappeared a few minutes after the arrhythmia ceased. B: detail of the start of ventricular fibrillation; note the ventricular extrasystoles prior to the start of fibrillation (arrows) and how this arrhythmia is set off by one of these. C: detail of the spontaneous ceasing of the ventricular fibrillation.
The VF that occurs in the absence of structural heart disease or electrocardiographic alterations is found in 5%-10% of survivors of sudden death,1-3 and is known as idiopathic VF (IVF). It is recurrent, it can be self-limiting and manifests in syncopes.1 Just as in atrial fibrillation, which can appear as a result of a focal mechanism with fibrillatory conduction, in some VF a trigger is identified that is a VE which sets off an arrhythmia. In the IVF, the VE has the same morphology and identical coupling interval and originates in the right ventricular outflow exit tract or in the Purkinje fibres.4,5 Besides in the IVF, it has been observed in patients with channelopathies (long QT and Brugada syndromes) and in certain patients with post-myocardial infarction scarring.6,7
In the treatment of IVF, medication is ineffective and until recently the handling of survivors was limited to the implanting of a defibrillator. Recently, Haissaguerre et al3 performed a radio frequency ablation of the VE which set off the IVF in 27 patients, with a rate of clinical success of 89% during a follow-up of 24 (28) months. This treatment has been included in the latest guidelines for sudden death secondary prevention.8 A limitation of this technique is that the VE cannot be reproduced to perform the ablation.
The peculiarity of this case is the clear documentation that a VF of close to 3 minutes can spontaneously end without causing death or sequelae and the inter-relation between the VF and the appearance and disappearance of its trigger.