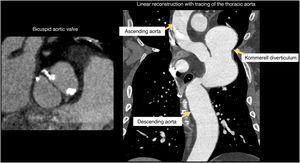
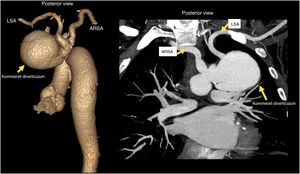
The present case concerns a 54-year-old man under follow-up by cardiology due to a bicuspid aortic valve and moderate stable angina with progressive worsening. Coronary angiography was performed but was nondiagnostic because the catheter could not be advanced beyond the aortic arch. Accordingly, the study was completed with coronary and aortic computed tomography, which revealed a bicuspid aortic valve and a Kommerell diverticulum aneurysm (longest axis, 6.6cm; figure 1), which was the origin of an aberrant right subclavian artery (ARSA) and the left subclavian artery (LSA) (figure 2). All pertinent informed consent was obtained. In addition, the patient had severe double vessel coronary artery disease with left-sided dominance and a hypoplastic right coronary artery, with a Coronary Artery Disease Reporting and Data System (CAD-RADS) 5 classification.


Aberrant right subclavian artery is an anatomical variant found in up to 1% of the healthy population that can have a small Kommerell diverticulum at its origin in 20% to 60% of cases. The Kommerell diverticulum can be asymptomatic or can have compressive symptoms affecting the trachea or esophagus. A literature review failed to identify patients with a Kommerell diverticulum of a similar volume and with origins for both subclavian arteries.
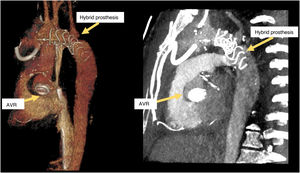
Due to its low frequency, management should be individualized; either open surgery or endovascular repair can be chosen. In the present case, we proposed aortic valve replacement (AVR) surgery with double coronary artery bypass and placement of a hybrid “frozen elephant trunk”-type ascending thoracic aortic prosthesis with transposition of the subclavian arteries (figure 3).
AUTHORS’ CONTRIBUTIONS
The authors contributed equally to this manuscript.
FUNDINGNone.
CONFLICTS OF INTERESTNone declared.