

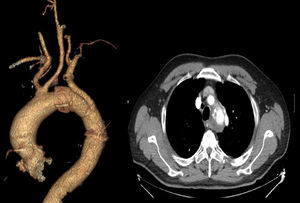
The present case concerns a 53-year-old man with a 4-month history of symptoms of dysphagia lusoria who attended our emergency department for chest pain. The patient was sweaty and hypertensive (210/100 mmHg). Electrocardiography showed sinus tachycardia without evidence of myocardial ischemia or altered repolarization. Urgent computed tomography ruled out acute aortic dissection but revealed a left aortic arch with bovine trunk, an aberrant right subclavian artery, and a Kommerell diverticulum (Figures 1 and 2) with a periaortic hematoma. Transthoracic echocardiography and coronary angiography were performed, with no abnormal findings. A 2-stage surgical intervention was indicated.


First, the right subclavian artery was transposed to the right common carotid artery. Second, via left thoracotomy and left heart bypass with extracorporeal circulation, the Kommerell diverticulum was replaced with a 26-mm Dacron graft and the left subclavian artery was reimplanted using an 8-mm Dacron graft (Figure 3). The presence of an aberrant right subclavian artery is an infrequent finding (0.2%-2.5%) but it has been seen to be the cause of aortic dissection complications and, as in this patient, the origin of a Kommerell diverticulum. Suspicion is based on the presence of dysphagia lusoria. The treatment for Kommerell diverticulum and aberrant subclavian artery is surgical, with excellent results. Endovascular treatment is a valid and recently introduced option.
