Keywords
See editorial on pages 1381-4
Received January 21, 2005. Accepted for publication June 10, 2005.
INTRODUCTION
Cardiac defects are the most common congenital malformations. The incidence in industrialized countries ranges between 5.2 and 12.5 per thousand live births. The range is so wide because the estimation of the incidence depends on many factors, such as inclusion criteria, diagnostic means, size of the population, duration of follow-up, etc. In fact, in a review published in 2002, Hoffman et al1 reported that the incidence of moderate and severe heart disease remains stable at about 6 per thousand, regardless of the place and time.
The objective of the present study was to determine the incidence and outcome of congenital heart disease in Navarra, a region in northern Spain with a population of somewhat more than half a million. An indirect assessment was made of the quality of the care offered to patients with congenital cardiac anomalies in this community in terms of diagnosis and treatment, taking into account the fact that heart surgery is not performed in the Community of Navarra and that children susceptible to invasive treatment must be transferred to another community.
PATIENTS AND METHODS
A retrospective study was performed in the population of Navarra, with 523 563 inhabitants, over a 10-year period. An exhaustive search for cardiac malformations was carried out in all the public and private hospitals and primary care centers of the Community of Navarra, and in the hospitals offering cardiac surgery outside of Navarra to which patients requiring invasive treatment are referred. The authors investigated the presence of cardiac malformations among the 47 783 children born in Navarra from 1989 to 1998.
"Cases" considered suitable for inclusion in this study were all children born in Navarra between 1 January 1989 and 31 December 1998. The factors considered in relation to cardiac malformation were the need for invasive treatments, associated arrhythmias and, finally, a family history of congenital malformations or, more specifically, cardiac malformations.
The SPSS statistical software package (version 10.0) for Windows was used in the statistical study of the results. The differences were considered to lack statistical significance when the P value was more than .05, while a value less than .05 was considered to indicate a statistically significant difference and less than .01, a highly significant difference.
RESULTS
Incidence
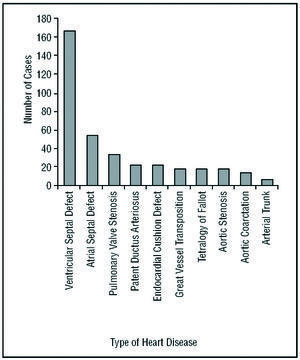
The incidence of congenital heart disease in the study population was 8.96 per thousand live births. The different types of congenital heart disease recorded appear in Table 1. Ninety percent of those diagnosed corresponded to the 10 most common types of cardiac lesions. The relative frequency of each is shown in Figure 1.


Figure 1. Most common forms of congenital heart disease.
Sex
Among the population presenting heart disease, there was a slight predominance of girls (51.9%) over boys (48.1%), although the difference was not statistically significant. All newborns were included, whether liveborn or stillborn, provided the gestational age was over 20 weeks. In some infants, the congenital heart disease was detected during the study period and, in others, later on. Data was collected up until 1 January 2003.
The definition of congenital heart disease was any anomaly in the heart or great vessels, among them, structural cardiac malformations, cardiac malposition not secondary to extracardiac malformations, congenital cardiomyopathy, and structural and vascular malposition not secondary to extracardiac anomalies. Atrial septal defects measuring less than 5 mm that closed prior to the age of 6 months, ductus arteriosus that closed during the first month of life (regardless of the gestational age), bicuspid aortic valve in the absence of aortic valve stenosis, mitral valve prolapse, cardiac malposition unaccompanied by structural heart disease and, finally, cardiac arrhythmias in the absence of other anomalies were excluded.
In the 428 children in whom congenital heart disease was diagnosed, the type of heart disease, the date and region of Navarra in which it was first detected, features of the delivery, and the diagnosis and course were studied. Among the children with patent ductus arteriosus, there was a highly significant predominance of girls (P=.003), who also presented a significantly higher incidence of ostium secundum atrial septal defect than boys (P=.014), while the latter predominated in the group with aortic stenosis (P=.041).
Prematurity and Data Concerning the Newborns
The incidence of prematurity (gestational age less than 37 full weeks) among infants with congenital heart disease was 15.9%. Twenty-two percent of them weighed less than 2500 g at birth, and 11.7% of these children had intrauterine growth retardation. The mean weight of newborns with cardiac lesions was 2983±696 g, the mean length was 48.7±3.3 cm, the mean head circumference was 33.88 cm and the mean chest circumference was 32.35 cm. The children with ostium secundum atrial septal defects were smaller in terms of weight, head circumference and chest circumference), while those with transposition of the great vessels were larger with respect to body weight and length.
The newborns with congenital heart disease presented mean 1-minute and 5-minute Apgar scores of 8 and 9, respectively. Cyanotic congenital heart disease (that presenting with clinical signs of cyanosis) were associated with a higher incidence of moderate and mild asphyxia (5-minute Apgar scores between 7 and 4), in comparison with noncyanotic disease (P=.005). The mean umbilical arterial and venous pH in newborns with congenital heart disease were 7.22 and 7.29, respectively. The umbilical cord arterial pH was lower in cases in which cyanosis was present (P=.048). Laboratory findings in 28% of the newborns with heart disease were indicative of acute fetal distress (umbilical cord arterial or venous pH less than 7.20).
Detection of Congenital Heart Disease
The cumulative detection rate of congenital heart disease at different frames was as follows: 1.27% were diagnosed prenatally, 25.3% on the first day of life, 45% during the first week of life, 65% during the first month of life and 83.1% during the first year of life. The detection rates presented here include all types of heart disease, both serious defects with early symptoms and less important lesions detected later on. The systematic use of echocardiography as a diagnostic tool has led to a highly significant increase (P<.01) in the detection of congenital heart disease (Table 2). Other diagnostic methods employed include diagnostic catheterization in 19.1%, magnetic resonance in 4.3%, scintigraphy in 1.2% and esophagography in 0.7% of the patients.

Of the ventricular septal defects detected, 55.4% resolved spontaneously.
Treatment of Congenital Heart Disease
Drug treatment was required in 8.4% of the cases of congenital heart disease at some point in time. The compounds employed were substances with cardiotonic, antiarrhythmic, vasodilator and diuretic activities.
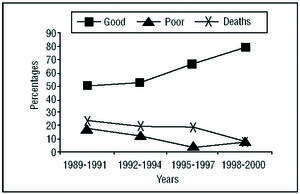
Invasive treatment was necessary in 30.8% of the cases: heart surgery in 25.4%, interventional catheterization in 6.4% and both approaches in 1%. The results were good (thus defined when they were satisfactory, although there remained a residual lesion of no functional importance) in 62% of the patients; fair (when the operation or catheterization did not achieve the objectives and there was only a slight improvement) in 10.8%; or poor (when the changes produced by the intervention were negligible) in 9%; and 18.4% of the children who underwent these procedures died, independently of the time elapsed between the intervention and death. Over the course of time, there has been a significant increase in the number of good results (P=.013) and significant decreases in the number of poor results (P=.018) and of postoperative deaths (P=.018), as can be observed in Figure 2.

Figure 2. Results of surgery and catheterization over time.
Mortality
The rate of cardiac-related mortality in patients with congenital heart disease was 10%. The Cardiac-related causes recorded were refractory congestive heart failure, cardiogenic shock, cardiorespiratory arrest, and, overall, the natural course of the heart disease itself, including the development of pulmonary hypertension. The mortality rate was significantly higher among patients with complete atrioventricular canal (P=.002) and patent truncus arteriosus (P=.017).
Arrhythmias
In 5.5% of the cases of congenital heart disease, there was an associated rhythm disorder, aside from those provoked by the surgery. The arrhythmias most frequently detected were premature beats, which constituted 26.9% of all the rhythm abnormalities. Wolff-Parkinson-White syndrome was present in 0.46% of the patients.
Family History
Among the relatives of these children, congenital malformations were recorded in 3.5% of the mothers, in 2.1% of the siblings and in 1% of the fathers. The congenital malformations most frequently detected were cardiac malformations, which were encountered in 3.5% of the mothers, 1.05% of the siblings and 0.5% of the fathers of the children with congenital heart disease. The similarity between the heart disease diagnosed in the child and that of his or her relatives was 50% with respect to both the mother and the father and 20% with respect to the siblings.
DISCUSSION
The incidence of congenital heart disease in Navarra is 8.96 per thousand live births. Owing, on the one hand, to the characteristics of the health care system of the Community of Navarra, where there is a referral hospital for heart disease in the pediatric population, and, on the other hand, to the method employed, in which the search for cases was done simultaneously in primary care centers (points from which patients are referred) and hospitals (points of reception), the resulting incidence rates of congenital heart disease among the population of Navarra, during the decade corresponding to the study period, closely approximate the theoretical real incidence. Few studies can guarantee such a strict monitoring of the population being evaluated. The incidence reported here falls within the range of values estimated in previous studies performed in the United States and Europe.1-23
In the present study, there is a slight predominance of women among the patients with heart disease, coinciding with a number of reports,6,11,24,27 while in other studies, the number of cases was higher among men10,14,19,22,28-31 or no differences between sexes were observed.32,33
The significant predominance of women observed in patent ductus arteriosus and in atrial septal defect has also been reported previously by other authors,30 as was the significant predominance of men among the patients with aortic stenosis.30,34
The percentage of newborns with congenital heart disease who were born prior to the 37th week of gestation also agrees with the findings in previous studies,6,28,35 and does not appear to differ significantly from that observed in the population constituted by full-term newborns.
The proportion of low-birth-weight infants with heart disease is 22%, an incidence similar to that reported in earlier studies,35,36 and that of newborns with heart disease presenting intrauterine growth retardation is 11.7%, a value similar to that detected by Kramer et al in the German population.36
With respect to the age of the child at the time of detection of heart disease, the diagnostic capability achieved in this study is similar to that reported elsewhere.6,7,14,20,22-25,28,30,32,37-43
The systematic use of echocardiography as a diagnostic tool has led to a highly significant increase in the detection of congenital heart disease (P<.01), a fact that has been demonstrated previously.5,7,22
In the present series, the utility of prenatal ultrasound in the detection of cardiac malformations was very limited, a circumstance that has been reported by other authors. This is due both to the low incidence of congenital heart disease in the general population and to the lack of familiarity with these conditions on the part of obstetricians, resulting in an inadequate evaluation of the fetal heart. The systematic use of fetal echocardiography has led to an increase in the rate of prenatal detection of congenital heart disease in Navarra.
The percentage of patients with heart disease who are treated surgically in this community is in agreement with rates reported elsewhere, which range between 14% and 33.3%.5,24,25,28,37,42,44-48 The proportion of cases of heart disease in which interventional catheterization is performed is also within the range of 2.8% to 19.7% that appears in the literature.37,44,48 The fact that the Community of Navarra does not offer interventional treatment (surgery or catheterization) has no influence on the number of interventions carried out or their outcome.
In this group of congenital diseases, the rate of mortality related to the heart disease itself is similar to, or even somewhat lower than, those reported by other authors.3,4,6,7,9,10,14,20,22,31,44,45,49-53
The postoperative mortality throughout the entire study is also in agreement with that of previous series,19,25,37,45,54-59 and, as time goes on, there is a significant decrease in this rate (P=.018).
It has been demonstrated that the relatives of children with congenital heart disease are at greater risk of presenting a structural cardiac lesion60 and that the risk is greatest among first-degree relatives. The present study detected a higher risk in the mother of the child with heart disease than in the father or siblings of said child.
It has also been shown that the rate of coincidence in the type of heart disease occurring in a given family is 17% to 60%.60,61 Here, the concordance between the type of heart disease presented by the child and that of his or her parents and siblings falls within the reported range, and is greater with respect to the parents than the sibs.
Table 3 shows the comparison of the results of this study with those published in the literature.

CONCLUSIONS
The incidence of congenital heart disease in the Community of Navarra, with 523 563 inhabitants, is 8.96 cases per thousand population. This incidence remained stable throughout the 10 years of the study.
Ninety percent of the cases of heart disease detected in this series were among the 10 most frequently diagnosed. They are, in descending order, ventricular septal defect, ostium secundum atrial septal defect, pulmonary valve stenosis, patent ductus arteriosus, transposition of the great vessels, complete atrioventricular canal, aortic valve stenosis, tetralogy of Fallot, aortic coarctation-aortic arch hypoplasia, and common arterial trunk.
In Navarra, from 1989 to 1998, the degree of suspicion and the diagnostic capability regarding congenital heart disease were high, ensuring an optimal detection of these anomalies in that region in recent years.
The results obtained with surgery and interventional catheterization are fully satisfactory and have tended to improve over the course of time, despite the fact that the Community of Navarra does not offer cardiac surgery and, thus, the children must be referred to other communities.
Correspondence: Dra. P. Martínez Olorón.
Servicio de Neonatología. Departamento de Pediatría. Hospital Virgen del Camino.
Irunlarrea, 4. 31008 Pamplona. Navarra. España.
E-mail: pmartino@cfnavarra.es