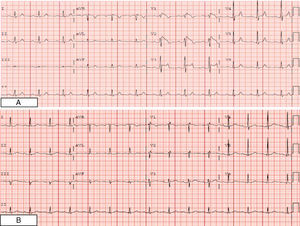
A 70-year-old patient with a history of hypertension and dyslipidemia was receiving treatment with enalapril, simvastatin, and hydrochlorothiazide. He was referred to our hospital for presyncope and suspected acute myocardial infarction in an anterior location. The first electrocardiogram (Fig. 1A) showed a saddlebag-type ST segment elevation in V1 to V3. Echocardiography excluded a segmental wall motion abnormality. Despite the patient's advanced age and the absence of previous episodes of syncope or a family history of sudden death, the presumptive diagnosis was Brugada syndrome. The initial analyses showed creatinine 4.88mg/dL, Na 127mEq/L, K 7.53mEq/L, pH 7.22, and troponin T <0.01ng/mL.

The patient was treated for hyperpotassemia and was hospitalized to investigate renal failure. Once the potassium concentration had normalized, a new electrocardiographic study was carried out (Fig. 1B), in which the Brugada pattern had disappeared. Nonetheless, a flecainide test was performed, with negative results. Various situations have been described in which an electrocardiographic pattern of Brugada syndrome is manifested, such as drug-related conditions, heart diseases, acute myocardial infarction with ST segment elevation, muscular dystrophy, and hypothermia. Although hyperpotassemia can display diverse manifestations on electrocardiography, a presentation mimicking a Brugada pattern is very unusual.
.