To the Editor,
We report the case of a 39-year-old homosexual male patient diagnosed through routine testing in 1998 as infected with human immunodeficiency virus type 1 (HIV-1). He had not developed any AIDS-defining disease and had no history of intravenous drug abuse, hepatitis C or B viral infection. His CD4+ T-cell count at the time of presentation was 758 cells/μL; the nadir CD4+ T-cell count was 512 cells/μL. Plasma RNA HIV-1 viral load was always undetectable (<50 copies/mL). He was treated with a fixed-dose formulation of 3 nucleoside analog reverse transcriptase inhibitors: zidovudine, lamivudine and abacavir (Trizivir®).
In August 2000 he suffered the first clinical manifestation of coronary artery disease (CAD) when he was admitted for an inferior ST-elevation acute myocardial infarction (STEMI). In August 2004, after a new anterior NSTEMI, his left ventricular ejection fraction was 20%. From this moment on, the patient developed progressive shortness of breath and symptoms of right heart failure. He required several hospitalizations despite optimized therapy, and was referred to our heart failure and heart transplantation (HTX) unit for evaluation. Right heart catheterization showed non-reversible pulmonary arterial hypertension (PAH) that precluded HTX consideration. Treatment with sildenafil citrate 20mg TID was initiated and gradually up-titrated to 100mg TID. After achieving target doses, a new right heart catheterization showed improved pulmonary resistance with reversible PAH. The pre-transplant study did not show any formal contraindication for HTX. Because of the patient's critical end-stage heart failure, young age, excellent response to combined antiretroviral therapy (cART) and lack of comorbidities, he was listed for HTX July 19, 2006. On September 7, 2007, the patient underwent successful elective orthotopic HTX.
The post-operative course was uncomplicated, standard induction was done with basiliximab 20mg within 24h of HTX and at 4days post-transplant. Routine immunosuppression treatment with methylprednisolone, tacrolimus and mycophenolate mofetil was initiated the day of surgery. The dose of tacrolimus required to achieve the target level of 10-15mg/dL was low during the first 6 months after transplantation (2mg daily) and increased with time to the standard dose (6mg daily). The cART was restarted on day 3 after HTX. Postoperatively, consistent improvement in PAH allowed the progressive withdrawal of sildenafil citrate until discontinuation.
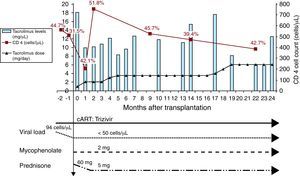
It is now 3years from HTX and the patient has improved remarkably. He has resumed work and leads an active life. Over this time, the patient had 1 episode, at 2 months after HTX, of acute rejection (International Society for Heart and Lung Transplantation grade 3A) requiring treatment with high-dose corticosteroids. Left heart catheterization at 1 year after HTX showed normal coronary arteries. He has not developed any focal or disseminated bacterial, viral, or fungal infection or any AIDS-defining disease. Weekly cytomegalovirus pp65 antigenemia testing was always negative. Under the cART regimen in addition to standard doses of immunosuppressant drugs, no pharmacokinetic interaction was detected. The CD4+ T-cell count evolution over time ranged between 201 and 754 cells/μL (Figure 1).

Figure 1. CD4+ T-cell count and percentage of lymphocytes, HIV-1 viral load, antiretroviral regimen and immunosuppressant drugs from heart transplantation to 24 months follow-up. cART, combined antiretroviral therapy.
The survival and quality of life in patients infected with HIV has dramatically changed since the introduction of cART in 1996.1 However, as HIV-1-related mortality decreases, cardiovascular diseases have become the primary cause of mortality in these patients. Antiretroviral regimes may cause dyslipemia, insulin resistance, and type 2 diabetes mellitus and have been associated to accelerated CAD.2 In this population, the incidence of CAD is increased 2-fold and the expected number of patients with end-stage heart failure secondary to ischemic heart disease is likely to increase. To our knowledge, ours is the first report of an HIV-infected heart recipient with ischemic cardiomyopathy. From the reported cases, 1 patient had advanced AIDS before HTX and survived only 3.5years after.3 The other 5 transplant recipients, similar to our case, were on cART regimes and had undetectable virus load, no AIDS-related manifestations, and uncomplicated post-operative courses. All of these patients suffered non-ischemic dilated cardiomyopathy.4
Although the first experiences with cardiac transplantation in very selected HIV-1- infected patients show very encouraging results, further reports and longer follow-ups are needed to elucidate possible HTX candidates when HIV infection coexists.
FundingPartially supported by the cooperating network of AIDS research teams of the Fondo de Investigación Sanitaria (FIS) and grant ISCIII-RETIC RD06/006 from the Instituto de Salud Carlos III, Madrid, Spain. Dr. J.M. Miró received a Research Grant from the Institut d’Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS).
Corresponding author: macastel@clinic.ub.es