
A 44-year-old man had undergone surgery with the Ross technique 8 years previously for a double rheumatic lesion of the aorta. He was currently being monitored for moderate homograft stenosis (maximum gradient of 60 mm Hg, 6 months earlier) detected 1.5 years after the procedure while he was in functional class 1. He had undergone a bilateral tympanoplasty 3 months previously for chronic bilateral cholesteatomatous otitis media.
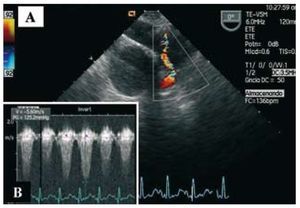
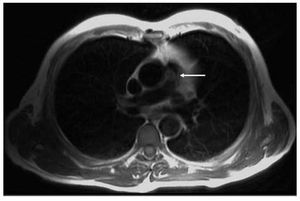
The patient came to the emergency room with a persistent fever of 20 days' duration, associated over the past 5 days with dyspnea and fatigue on minimum minimal exertion. He was admitted to the cardiology department; serial blood cultures isolated Streptococcus viridans. Transesophageal echocardiography showed a mildly dysfunctional dilated right ventricle, with a round, slightly mobile image on the pulmonary trunk (homograft), indicative of an endocarditis vegetation that considerably increased the pre-existing stenosis (Figure 1A); the maximum transpulmonary gradient was 125 mm Hg (Figure 1B). Magnetic resonance imaging was performed to provide better anatomic definition and tissue characterization of the homograft and lesion (Figure 2, arrow).

Figure 1.

Figure 2.
Following 1 month of treatment, the patient's functional class improved and the follow-up echocardiogram showed a reduction in the size of the vegetation and the transpulmonary gradient, which was recorded at 70 mm Hg. Nevertheless, the persistent low-grade fever and severity of the valve lesion ultimately required replacement of the affected graft, from which the vegetation was separated (Figure 3).

Figure 3.