
To the Editor,
Although 20%-55% of people with Whipple's disease present cardiac involvement,1 the episodes of endocarditis due to Tropheryma whipplei are uncommon,2-5 and thus this agent is rarely taken into account during etiologic differential diagnosis when endocarditis is suspected but hemocultures are negative.
We present a patient treated in our hospital, where the suspected initial diagnosis was infective endocarditis (IE) with hemocultures negative for papillary fibroelastoma on the native aortic valve. Endocarditis due to T. whipplei was later diagnosed by PCR analysis.
This 57-year-old woman without known heart disease has a prolonged history of polyarthralgias, pretibial pain and peripheral neuropathy classified as palindromic rheumatism, long-term hypertransaminasemia, chronic cough with negative functional and allergy tests, transient episodes of diplopia and frequent headaches, without diarrhea or other clinical digestive disorders, and had received oral corticoid treatment only. She was admitted to the cardiology unit due to congestive heart failure. During examination she had no fever, but did present enlarged latero-cervical lymph nodes and grade II/ IV diastolic murmur in the right parasternal border.
The echocardiogram showed a 1.2-cm mass on the left coronary aortic leaflet that caused severe aortic regurgitation (Figure 1). Hemocultures were taken but the results were negative.

Figure 1.Transesophageal echocardiogram showing a 1.2 cm mass from the aortic valve.
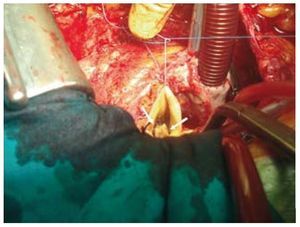
Given the suspicion of IE with negative hemoculture for papillary fibroelastoma, surgical treatment was prescribed. During the intraoperative phase, large fibrous adhesions were found in the pericardium and a mass with a polypoid appearance (1.2´0.5 cm) was confirmed in the aortic face of the left coronary leaflet (Figure 2). The valve was resected and replaced with a mechanical prosthesis.

Figure 2.Polypoid mass on the left coronary leaflet of the aortic valve.
No microorganisms were found in the pericardial and aortic valve cultures, but a subsequent general PCR analysis isolated T whipplei in pericardial and valvular tissue.
Given the diagnosis of T whipplei endocarditis, antibiotic treatment with ceftriaxone IV was given for 1 week, followed by oral trimethoprim-sulfamethoxazole. The patient was admitted 1 month after hospital discharge for nausea and food-associated vomiting due to prerenal acute kidney failure.
At a subsequent check-up the patient demonstrated functional class I, with a normally functioning prosthesis and substantial improvement in lumbar and ankle pain; the only persistent problem was intermittent right-knee pain. The patient does not present diarrhea or other digestive clinical symptoms. Currently, she is still receiving antibiotic treatment with oral cotrimoxazole that will be maintained for at least 18 months.
The first case of her diagnosed disease was described in 1907 by Whipple,6 who called it intestinal lipodystrophy. In 1952 the first effective guideline of antibiotic treatment was achieved. In 2000, the causal bacillus was successfully isolated and cultivated and in 2003 the full sequence of the genome was analyzed.
The main symptoms consist of arthralgias, weight loss, diarrhea and abdominal pain, although other parts of the body can also be affected, such as the central nervous system, lungs, and heart. The incidence of this disorder is around 30 new cases per year. It is more common in men (86%) than in women.7 If treatment is not received, the disease is lethal.
There is cardiac involvement in 20%-55% of the cases1 of the Whipple's disease and can affect all the layers of the heart. It can occur with thoracic pain and pericardial friction, interstitial myocarditis and endocarditis, and is more common on the mitral valve than on the aortic valve. Endocarditis due to T whipplei has also been described on a mitral valve bioprosthesis.8
Treatment consists in valve replacement and long-term antibiotic treatment (around 1-2 years) with trimethoprim-sulfamethoxazole; no recurrences have been described.