To the Editor:
During the summer of 2006, we climbed the Galician section of El Camino de Santiago ("Route of Santiago") together with 21 low-risk coronary patients and their partners, using this legendary goal to encourage these patients to undertake a rehabilitation program in a leisure setting and as a physical and psychological challenge. The basic idea of the initial experience was to explore the safety, accessibility, and possibilities of the program.
Twenty-one patients who met the conditions required by the Preventive Cardiology and Rehabilitation Section of the Sociedad Española de Cardiología (Spanish Society of Cardiology) for low-risk patients signed the consent form.1 All participants (patients and partners) were advised to undertake a walking program 2 months before the starting date. This program included 5 kilometers a day during the first month and 10 kilometers in the second, as well as determinations of blood sugar, lipids, blood pressure, and weight before and after the event (Table 1). All individuals completed 4 surveys to assess their psychological profile, knowledge of disease, risk factors, and heart-healthy lifestyle habits, as well as their use of the various food groups. The data obtained were then used in a series of discussion talks held to enhance the patients' knowledge in these areas.

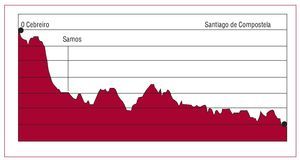
For safety and support purposes, we had a physician and 2 nurses, a logistic support car, and another medical care vehicle to carry medication, cardiac arrest equipment, a defibrillator and oxygen cylinder, and finally, a bus to connect the starting and ending points for the different stages with a hotel located in Sarria, where the discussion talks were held. The following route was taken (Figure 1):

- Stage 1. O'Cebreiro-Triacastela. We skipped the first 8.5 kilometers to avoid 2 climbs without a warm-up that ended at the Poio summit (altitude, 1280 m above sea level). From there, we walked 12.5 kilometers, initially on flat ground, followed by a descent to Triacastela (660 m above sea level)
- Stage 2. Triacastela-Sarria (440 m above sea level). We walked toward Samos for 18.6 kilometers, avoiding the first 4 kilometers that run parallel to the road because they required reaching the top of a peak at kilometer 4.7 and had difficult sections for the support vehicles. We felt that the next section, Sarria-Portomarín, was inappropriate, with too many parts unsuitable for vehicular traffic
- Stage 3. Portomarín (350 m above sea level)-Palas de Rey (5650 m above sea level), 23 kilometers. This is very rough terrain with an initial climb toward the Gonzar road (540 m above sea level), followed by a flat section of 4 kilometers and 2 more climbs to reach 700 m above sea level and another downhill section, and another climb to cross the Ligonde mountain range (580 m above sea level). This orography can disrupt the discipline of the gait and cause angina crises
- Stage 4. Palas de Rey-Melide (455 m above sea level), 15.7 kilometers, and 5th stage, Melide-Arzúa (390 m above sea level), 13.6 kilometers. These stages run over hills and valleys crossed by 6 rivers that empty into the Ulla, with a continuous up-and-down path that tires the climber, and results in safety problems. Some sections pose difficulties for vehicular traffic
- Stage 6. Arzúa-Arca (305 m above sea level), 18 kilometers, and stage 7, Arca-Monte del Gozo (345 m above sea level), 15.7 kilometers, flat and with no problems
All patients completed the route successfully with no incidents. Therefore, we consider that the route is appropriate for the needs of the program when precautions that place a high priority on safety are incorporated.
We believe that this experience has many positive aspects: a) it proposes a challenging goal that would normally be unthinkable and therefore can enhance the patient's confidence in his or her physical and psychological capabilities; b) it is undertaken with similar patients, which allows synergies to be established that help achieve the objectives; c) it includes a touristic element as a pleasant addition to the program and represents an ideal setting for social interaction among the participants and for the training activities; d) it includes the participation of the patients'partners, which can help mitigate the adverse aspects of cardiac disease on the social and family environment and help to achieve heart-healthy practices; and e) it attempts to convey a message to patients and the general population about leading a normal life that may help demystify the limitations of this disease.
Subsidized by the Ministry of Health of the Community of Madrid, FROM (Ministry of Agriculture, Fisheries, and Food), and Laboratorios Pfizer.