To the Editor:
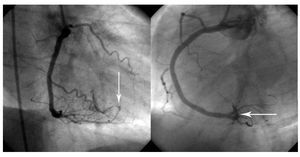
We present the case of a 42-year-old man admitted to our hospital for non-Q-wave acute myocardial infarction. Following treatment with aspirin plus clopidogrel, enoxaparin, atenolol, and nitroglycerin, early elective coronary angiography was performed and a severe, long, irregular stenotic lesion was found in the middle segment of the right coronary artery. Because of the anticipated difficulty for crossing the lesion, a hydrophilic angioplasty guidewire (PT Graphix, Boston Scientific, United States) was chosen. Direct implantation of a sirolimus-eluting stent (Cypher, Cordis Inc, United States) was tried; however, when attempting to cross the lesion with the device, the guidewire was displaced toward the ascending aorta, dragging along the guide catheter, which had to be advanced toward the septal branch of the posterior interventricular artery. A 3´24-mm stent was then implanted in the middle segment by inflation at 13 atmospheres for 30 seconds. Following withdrawal of the guidewire, a fistula appeared between the septal branch and the right ventricle (Figure 1). There were no hemodynamic symptoms or abnormalities. The patient progressed satisfactorily during the hospitalization. Echocardiography identified and located the fistulous tract (Figure 2), which was draining into the right ventricle at a rate of 3 m/s. No evidence of volumetric overload of the right chambers was observed and repeated measures of Qp/Qs were around 1.1. Therefore, the patient was discharged home with conventional treatment.

Figure 1. Right and left anterior oblique angiographic views that show extravasation of contrast material from the septal artery arising from the posterior interventricular artery toward the right ventricular chamber.

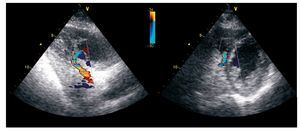
Figure 2. Modified (left) longitudinal apical echocardiographic view in which color Doppler reveals a section of the posterior interventricular artery and septal artery with accelerated flow and the communication with the right ventricular chamber. Transverse (right) parasternal view shows the site of the defect at the junction of the inferior septum and the right ventricular free wall.
The 2-month follow-up showed complete and spontaneous closure of the fistula.
The complication described herein is a problem observed rarely, but not exceptionally, after insertion of hydrophilic guidewires.1 Perforation of the epicardial coronary arteries occurs generally toward the pericardial sac,2 with the consequential risk of cardiac tamponade that requires immediate treatment.3 In this case, drainage to a ventricular chamber and the intramyocardial path of the culprit artery are factors that decreased the patient's risk of acute hemodynamic instability. The potential late complications of this situation include progression of left-to-right shunting, pulmonary hypertension, high output heart failure, and distal ischemia in the artery affected by steal phenomenon.
Closure has been recommended for large fistulae with hemodynamic abnormalities, whether by surgery (which usually requires extracorporeal circulation, percutaneous embolization with coils, or closure of the native artery by stents of impermeable material.4,5 Conversely, small fistulae tend to follow a benign course.6
The appropriate treatment for this problem has still not been established and should be individualized according to severity.7 In this case, clinical and echocardiographic observation was chosen, and spontaneous resolution was confirmed.