
To the Editor,
Abdominal aortic aneurysm (AAA) affects 1.5%-2% of the general adult population and 6%-7% of those over 60 years, and its incidence is increasing1 due to ageing and atherosclerosis (associated with 75% of cases); up to 91% of AAAs affect the infrarenal aorta. Its risk factors include being aged over 60 years, male gender, smoking, hypertension, family history of AAA and atherosclerosis (coronary, peripheral or cerebrovascular).2 There is also a genetic predisposition, affecting up to 30% of first-degree relatives.
Although 75% of AAAs are asymptomatic and are found by chance on an imaging test, its complications can be fatal, especially its rupture, which has a 60% pre-hospital mortality and 50% for those who undergo emergency surgery (total mortality, 85%).1-3
Therefore, early diagnosis of AAA has important therapeutic prognostic implications for allowing elective reconstructive surgery or planning its control, thus reducing its morbidity and mortality. Although abdominal ultrasound is the technique of choice for diagnosis, monitoring and screening for AAA1-3 over various studies in different populations at risk has found that during conventional transthoracic echocardiography (TTE) all the abdominal aorta can be studied2,3: the suprarenal by subcostal access and infrarenal with bifurcation by placing the transducer at the left paraumbilical level (with the patient supine) or right paraumbilical (with the patient semisupine on left side, with less interference from intestinal gas). The abdominal aorta is shown in more than 95% of cases, and it is estimated that AAA is detected in up to 3%-5.7% of the TTEs performed for any reason.1,2
This study, which requires no additional equipment and increases total exploratory time by less than 5 min.1-3
For example, we describe the case of 2 patients admitted for acute myocardial infarction:
- A 72-year-old woman with cardiovascular risk factors and ischaemic heart disease. After studying the abdominal aorta during TTE (for sub-costal and paraumbilical access), a large aneurysm was seen of the entire abdominal aorta, 6.5´5.5 cm, calcified with severe circumferential mural thrombosis and effective diameter <2.6 cm in diameter (Figure 1). A CT scan confirmed the findings.

Figure 1. A: echocardiography, aneurysm of the infrarenal abdominal aorta, calcified and thrombosed (arrow). B: CT scan with contrast, cross-section. C: coronal sections. D: sagittal sections.
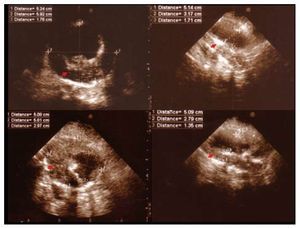
- A male patient, 68 years old, smoker, dyslipidemic with severe ischaemic heart disease. After performing the final aortic study during the TTE (subcostal access and paraumbilical), an AAA infrarenal of 5.8´5.1 cm was seen with severe and calcified eccentric mural thrombosis and a fresh, mobile thrombus attached that left an effective aortic diameter of <2.7 cm (Figure 2).

Figure. 2. Aneurysm of the infrarenal abdominal aorta, calcified and thrombosed.
Several studies have shown that screening for AAA in the general population is not cost-effective. Therefore, it has been advised to study only those patient groups where the incidence of AAA is greater. In short, we can define 2 populations for screening1,2: a) males over 50 and women over 65 years and b) those with risk factors associated with AAA.
In recent recommendations on TTE, The European Association of Echocardiography cited previous documents in which the aorta is scarcely evaluated and the focus is only on subcostal access.4
No explicit recommendation was made, despite the ease, low cost, speed, and paraumbilical access during ETE, as well as the usefulness of studying the entire abdominal aorta, as shown by the clinical cases. AAA screening is proposed in patients who are being studied by TTE for any reason, and who belong to one of the two populations at risk. This aortic study should be performed by the 2 ultrasonography entries described.
The study of the abdominal aorta permits us a more comprehensive assessment of cardiovascular disease in our patients, allowing us to gain diagnostic autonomy and learn more about aortic and atherosclerotic disease. Evaluation of AAA can be completed with other radiological techniques such as abdominal ultrasound.