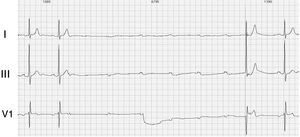
A 75-year-old woman was admitted to our hospital for several syncopal episodes in the last 2 weeks. Until then, the patient only had hypertension, which was well treated with angiotensin-converting enzyme inhibitors. Cardiopulmonary examination showed bilateral air entry and normal heart sounds with a mild aortic systolic murmur. There was no peripheral edema. During hospitalization, she underwent 24-hour electrocardiographic recording. Her baseline 12-lead electrocardiogram (ECG) showed sinus rhythm, first degree atrioventricular block (PR interval 220 ms), and incomplete right branch block. During the night, some episodes of paroxysmal III degree atrioventricular block were observed. The ECG in figure 1 shows complete atrioventricular block occurring during the morning (11:37 AM), immediately after a nonconducted premature atrial beat. AV conduction recovered after a junctional ectopic beat. The patient underwent dual chamber pacemaker implantation and was discharged 2 days later.

What is the mechanism underlying paroxysmal atrioventricular block?
- 1.
Vagal hypertonia.
- 2.
Phase 4 paroxysmal atrioventricular block.
- 3.
Pseudo-atrioventricular block due to concealed junctional extrasystoles.
- 4.
Phase 3 paroxysmal atrioventricular block.
Submit your answer to http://www.revespcardiol.org/en/electroreto/73/11. The answer will be published in the next issue (December 2020). #RetoECG.