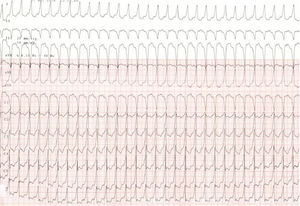
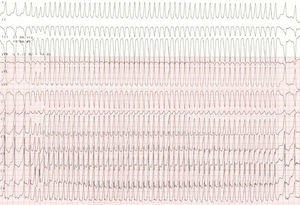
A 60-year-old man, institutionalized for chronic alcohol abuse, was admitted to the emergency room of our hospital with asthenia, dyspnea, and worsening edema. The patient was not experiencing palpitations, syncope, or chest pain. The electrocardiogram performed on admission showed regular broad QRS tachycardia at a rate of approximately 160 bpm (Figure 1). Vagal maneuvers elicited no response. On endovenous administration of a 12mg adenosine bolus, transient acceleration of the tachycardia was observed, as shown in Figure 2. The echocardiogram showed severe biventricular dysfunction and no intracavitary thrombus. The tachycardia finally resolved with electrical cardioversion.


What do you think was the most likely diagnosis?
- 1.
Idiopathic posterior fascicular ventricular tachycardia
- 2.
Pre-excited atrial flutter
- 3.
Supraventricular paroxysmal atrioventricular node reentry tachycardia
- 4.
Atrial flutter with aberrant conduction
Submit your diagnosis at http://www.revespcardiol.org/es/electroreto/72/03. The diagnosis will be published in the next issue (April 2019). #ECGChallenge.