A 47-year-old-woman with an unremarkable medical history was admitted to hospital for nonspecific central chest pain of 1 month's duration, fever, and asthenia. The physical examination and electrocardiography study showed no abnormal findings. The hemogram and myocardial injury markers were normal, as were serologies for cytomegalovirus, Epstein-Barr virus, hepatitis B and C virus, human immunodeficiency virus, Coxsackie virus, and bacteria (syphilis by rapid plasma reagin, Brucella, Lyme disease). Inflammatory markers were elevated (erythrocyte sedimentation rate, 103 mm/h and C-reactive protein, 56 mg/L). There were no abnormal findings on echocardiography.
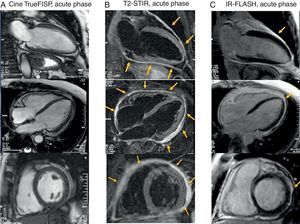
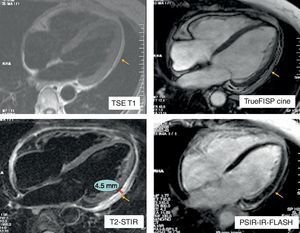
Magnetic resonance imaging showed preserved left ventricular size and contractility, and generalized pericardial thickening that was more marked in the basal segments (5.5 mm) than in the apical segments (4.5 mm), with no effusion and no evidence of constriction on tagging sequences. Sequences acquired in the acute phase (Fig. 1) depict increased pericardial thickness with no effusion (cine, Fig. 1A), increased signal intensity in both pericardial layers indicating inflammation with extensive edema (short time inversion recovery sequences [STIR], Fig. 1B), and late gadolinium enhancement, consistent with pericardial inflammation. Concomitant myocardial involvement was ruled out (inversion-recovery sequences, Fig. 1C). Figure 2 illustrates the possibilities of magnetic resonance to measure pericardial thickening with different sequences.


A diagnosis of acute, dry pericarditis was established, and the patient was treated with anti-inflammatory therapy for 4 weeks.
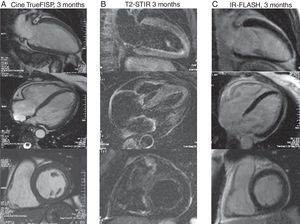
A follow-up cardiac magnetic resonance study was performed 3 months later (Fig. 3). STIR sequences showed complete resolution of the pericardial edema (Fig. 3B), with sight persistence of late gadolinium enhancement (Fig. 3C), typical features of this condition after the acute phase.
