Acromegaly is a disease characterized by chronic growth hormone (GH) hypersecretion.1 Cardiovascular alterations such as hypertension (HT), left ventricular hypertrophy, and ischemic heart disease are common in this condition and represent the main cause of death.2 Nevertheless, dilated cardiomyopathy is rare, and on occasions it is difficult to attribute its origin to a direct effect of GH on the heart, due to the frequent coexistence of other possible causes.
We describe a patient with acromegaly and dilated cardiomyopathy who presented ventricular contractility and diameter normalization following treatment with a somatostatin analog.
The patient was a 61-year-old woman with a history of type 2 diabetes mellitus, hypercholesterolemia, hysterectomy plus double adnexectomy, and severe obstructive sleep apnea syndrome (OSAS). She had been diagnosed three years earlier with dilated cardiomyopathy with angiographically normal coronaries and severe ventricular dysfunction, and was being treated with carvedilol 25 mg, low-dose digoxin, ramipril 2.5 mg, spironolactone, and statins.
The physical examination showed a blood pressure of 120/60 mm Hg and excess weight; pulmonary auscultation was normal and cardiac auscultation was rhythmic, with a Grade 1/6 ejection systolic murmur. The analyses showed a glucose level of 148 mg/dL; all other biochemistry, coagulation, and blood count results were normal.
The electrocardiogram (ECG) was in sinus rhythm at 40 bpm with left bundle-branch block, and the chest x-ray disclosed cardiomegaly.
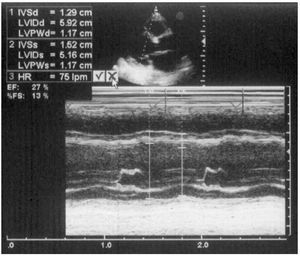
Echocardiography performed 2 years before showed a left ventricular end-diastolic diameter (LVEDD) of 59 mm and left ventricular ejection fraction (LVEF) of 22% (Figure 1).

Figure 1. Two-dimensional echocardiogram at baseline with large ventricular diameters and generalized left ventricular hypokinesia.
In view of the development of diabetes mellitus and the presence of coarse physical traits, GH levels had been measured 15 months earlier and were found to be elevated. Magnetic resonance imaging of the pituitary gland showed a microadenoma on the left, near the cavity.
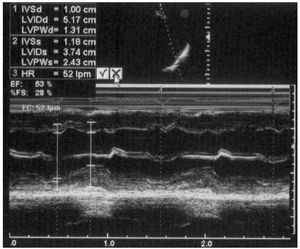
Fourteen months before the current visit, treatment was started with a somatostatin analog. At the 4-month follow-up from the start of treatment, echocardiography showed LVEDD 57 mm and LVEF 35%; at 14 months, LVEDD was 52 mm and LVEF, 56% (Figure 2). Following treatment, left bundle-branch block persisted on echocardiography. A reduction in the levels of GH and its mediator, IGF-1, and a decrease in the size of the microadenoma with respect to the baseline study were also seen.

Figure 2. Two-dimensional echocardiogram after 14 months under treatment with a somatostatin analog, showing normal left ventricular diameter and contractility
Cardiovascular disease, in particular, ischemic heart disease, is the main cause of death in patients with acromegaly.2 The condition tends to induce left ventricular hypertrophy, regardless of the presence of hypertension, and is sometimes accompanied by myocarditis with lymphomononuclear infiltration, areas of monocyte necrosis, and proliferation of the collagen component.3,4 Possible valvular involvement, with mitral and tricuspid prolapse, has also been described.5
The high prevalence of ECG and echocardiographic alterations in acromegalic patients (60%-70% according to some publications) has led some authors to recommend routine cardiologic study in these patients, even when they are asymptomatic.2-4
Dilated cardiomyopathy, although rare, is possible in the long-term evolution of acromegaly. The presence of major physical traits in our patient supports the diagnosis of acromegaly from many years earlier.
Due to the high prevalence of hypertension, diabetes mellitus, and hyperinsulinism in acromegalic patients, some authors have questioned the presence of an authentic "acromegalic cardiomyopathy," ie, secondary to the direct effect of excess GH on the heart.6 However, Marín Ortuño et al7 observed a high prevalence of diastolic involvement of the right ventricle (not subjected to increased afterload) in acromegaly. This data provides evidence for a direct effect of GH and/or its mediator, IGF-1, on the heart. High blood pressure and ischemic heart disease were ruled out in our patient as possible causes of dilated cardiomyopathy, and other causes (such as viral or toxic) are more difficult to prove.
Current consensus recommends surgery as the treatment of choice for acromegalic cardiomyopathy,8 although clinical, echocardiographic, and even histopathologic improvement has been shown after treatment with subcutaneous octreotide.5,6 Our patient was treated with somatostatin analogs, drugs that improve acromegalic cardiomyopathy9,10 and reduce or normalize GH and IGF-1 levels in a high percentage of cases; the effect is observed within a few weeks, is reversible, and is not associated with hypopituitarism.11
The case we present is one of the few described in which a patient with dilated cardiomyopathy was treated with octreotide as an initial option, with improvement in cardiac dilation and ventricular function.