Keywords
INTRODUCTION
The American Diabetes Association recently defined diabetes mellitus (DM), particularly type 2 DM, as a generalized cardiovascular disorder of metabolic origen.1 Although several studies have shown the important micro- and macro-angiopathic consequences of DM, the quantitative degree in relation to ischemic heart disease is not clear. Some authors have equated death from diabetes with death from stable ischemic heart disease,2-5 though others have reported a lower rate.6 Whatever the situation, the presence of diabetes and its duration are both independent risk factors for total and cardiovascular mortality in various populations and groups.7-9 This high rate of death and disease and the ever increasing frequency of diabetes in our environment10 led to the creation of a Working Group on the Heart and Diabetes, within the scientific scope of the Spanish Society of Cardiology, to examine the cardiovascular consequences of DM. One of the activities of this group was to examine the clinical reality of DM, relative to the clinical and numerical consequences as well as to the therapeutic approaches applied by cardiologists. Accordingly, a survey was mailed to all cardiologists who were members of the Spanish Society of Cardiology. The results of this survey form the basis of this report.
METHODS
A transverse study was undertaken based on the collection of responses to a survey mailed to all 1840 cardiologists who were members of the Spanish Society of Cardiology in 2001. The survey was designed by the specialist company Dendrite-Synavant, which was entrusted with its production, postal distribution and anonymous analysis of the responses. The survey, which could be answered anonymously, consisted of 16 questions with various possible responses, as well as the possibility of making any opportune comments. The data are expressed as percentages of responses selected from those available for each question. No statistical analysis was planned because of the descriptive nature of the study.
RESULTS
The survey, mailed to 1840 cardiologists who were members of the Spanish Society of Cardiology, was answered by 348 (18.9%). The questions included in the survey concerned different aspects of the management of DM by cardiologists and the results will therefore be presented in different sections. Table 1 summarizes the percentage of responses to each of the questions.

Organizational Aspects
The creation of a specific working group on the heart and diabetes was judged necessary by 90.2% of the responders and 63.8% stated their knowledge of diabetes was inadequate. Some thought this was due to insufficient training in this topic during the period of specialization and lack of later reinforcement. One quarter (25.3%) of those who responded considered that insufficient importance was given to DM in the different scientific meetings and publications of the Spanish Society of Cardiology, whereas 28.2% on the other hand thought this was sufficient and adequate. The responses were more varied in their opinions as to how to improve the cardiologists' knowledge of DM: 34.2% indicated the need to establish a new consensus on DM and cardiovascular disease, so that agreements with other relevant specialists would result in schemes and guidelines for medical action which would improve clinical practice; 23.5% thought the regular organization of continuing medical education courses would suffice; 22.1% thought a specific section should be created in the Revista Española de Cardiología dealing with the heart and diabetes, and finally, 20.2% considered that periodical publications left to the criteria of the editorial committee would be sufficient. Another important aspect was that 82.5% of the responders considered that the cardiologist should be better informed in the management of oral antidiabetic agents and insulin.
Clinical Aspects
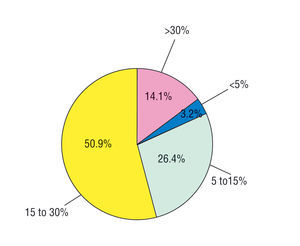
Concerning the prevalence of DM in the cardiologic setting, half the responders said that 15%-30% of the patients they see with heart disease also have diabetes. One quarter of the responders placed this prevalence at 5%-15%, whereas 14.1% thought it was above 30%. Only 3.2% of the responders considered that fewer than 5% of their patients were also diabetic (Figure 1).

Fig. 1. Prevalence estimated by the responders of the percentage of their cardiologic patients who have diabetes.
Evaluation of the clinical and analytical workup undertaken by the cardiologist to determine the metabolic status of the patient showed that baseline glycemia was requested by 93.1% of those who responded, glycosuria by 40.8%, an oral glucose tolerance test by 13.5%, glycosylated hemoglobin by 75.9%, microalbuminuria by 59.2%, and other parameters (uric acid, albumin, fructosamin, liver function, thyroid function, homocysteine, reactive C protein) by 25.9%.
The cardiologists were asked at what point they requested a consultation with the specialist in DM after first detecting some carbohydrate disorder (baseline glycemia >126 mg/dL, oral glucose tolerance test at 2 hours >140 mg/dL or glycosylated hemoglobin >6.5%) in their patients with heart disease. Forty-three percent of the cardiologists responded that they requested the consultation immediately, 88.0% did so after unsuccessfully attempting to normalize the situation with dietary and lifestyle changes, 58.0% directly started therapy with oral antidiabetic agents and 34.0% started insulin therapy. Thirty-five point seven percent of the responders understood that they should request the advice of an endocrinologist in all cases, 33.8% only if the diabetes was difficult to control, and 30.7% only if the baseline glycemia or glycosylated hemoglobin could not be controlled with non-pharmacologic measures. On the other hand, only 23.6% considered they were sufficiently familiar with oral antidiabetic agents, and even fewer (15.5%) with the use of insulin. Reciprocally, 72.3% of the responders considered that the endocrinologists only consult the cardiologists if there is manifest evidence of heart disease in their diabetic patients, 10.3% always consult the cardiologist, and 10.9% never.
Regarding the clinical tests generally used for the diagnosis of cardiovascular complications of diabetes, 96.0% perform a baseline electrocardiogram, 46.0% a simple exercise test, 10.0% a radioactive isotope study, 49.0% a Doppler echocardiogram, 4.0% a stress echocardiogram, 4.0% an ambulatory electrocardiographic recording, 6.0% an ambulatory blood pressure follow-up and 3.0% coronary angiography.
Therapeutic Aspects
Sixty-five point eight percent of the members of the Spanish Society of Cardiology consider that the primary prevention given to the patient with diabetes but with no apparent heart disease is not the same as that for coronary patients. Regarding the primary prevention treatment used in the diabetic patient with no manifest cardiovascular complication but with some associated risk factor, such as hypertension, smoking, obesity or dyslipidemia, 87.6% use angiotensin converting enzyme inhibitors, 86.2% use aspirin, 91.4%, statins, 44.3% angiotensin AT1 receptor antagonists, and 12.2% other drugs, such as beta-blockers, calcium antagonists, or diuretics. Finally, whereas 57.8% of the responders consider the cooperation of the cardiologist in hospital metabolic units to be absolutely necessary, 33.1% only consider this cooperation necessary occasionally and 7.8% do not consider it expedient at all.
DISCUSSION
Diabetes mellitus is a group of extraordinarily prevalent metabolic diseases which induces important deterioration of the cardiovascular apparatus as a result of its micro- and macro-angiopathic complications.3 The prevalence of DM is increasing and the number of persons in the world with type 2 DM is expected to double in the next 10 years. Furthermore, the more developed the country and the greater the life expectancy, the more evident this prevalence will be. As the presence of DM results in a 2-4 fold increase in cardiovascular risk, cardiovascular complications will consequently constitute a major general health problem. The prevention, diagnosis and treatment of cardiovascular complications of DM are therefore incumbent on cardiologists, in close collaboration with epidemiologists, endocrinologists, internists and family physicians.11
Organizational Aspects
The results of the study presented in this report are based solely on the responses to a survey. Nevertheless, they reflect aspects which illustrate well the views of Spanish cardiologists concerning DM and its cardiovascular consequences. Although the response rate did not reach 20%, those who did answer can be considered to form a group interested in the problem and whose opinions are of great relevance. Moreover, free surveys very rarely result in much higher response rates than the rate seen here.
Most of those who responded consider opportune the creation of the Working Group on the Heart and Diabetes within the scientific structure of the Spanish Society of Cardiology. In general, the dominant opinion was that the knowledge of cardiologists concerning the management of patients with diabetes is definitely insufficient. Although this fact may seem somewhat disappointing, it is nevertheless stimulating and obliges us to set up those resources necessary to increase our knowledge of this very prevalent and severe cardiovascular risk factor.
Half the cardiologists who responded to the survey considered that our scientific structure should take more interest in this disease, resorting to any valid form to do so. Only a very small percentage of responders felt satisfied that the way the Spanish Society of Cardiology dealt with the disease is already adequate. One third of those surveyed felt that a new consensus on DM and cardiovascular disease which would clearly contribute to decision taking should be established to improve the cardiologists' knowledge of DM. The remainder were divided in their opinions and preferred either continuing medical education courses, regular publications, or the creation of a special section in the Revista Española de Cardiología dealing with the heart and diabetes. The data obtained from this survey are not very different from those reported in similar surveys, such as the joint Canadian and American National Health Surveys12 and the German experience.13
Diagnostic Aspects
The interest of cardiologists in DM is truly stimulating, judging by the medical tests requested to determine the metabolic status of their patients. In order of importance, these tests were baseline glycemia (94%), glycosylated hemoglobin (76%), proteinuria (76%), and renal function and glycosuria (59%). However, the resulting therapeutic decision is not uniform. Given a diagnosis of carbohydrate metabolism disorder, half the cardiologists treat the disease directly and half refer the patient to the endocrinologist.14-16
Of those who treat the patient, almost all advise changes in lifestyle and a suitable diet. Only half those surveyed decide to initiate therapy with oral antidiabetic agents if necessary and only one third feel prepared and sure enough to manage insulin therapy. The most important tests used by the cardiologist in patients with diabetes but with no apparent heart disease are baseline ECG (96%) and a simple exercise test (46%).
Treatment
Sixty-six percent consider the secondary prevention used in coronary patients to be clearly superior to that applied to diabetic patients. This contrasts with the recommendations based on recent well-documented reports, which recommend that primary prevention of the diabetic patient with no apparent heart disease should be the same as that applied to patients with a prior myocardial infarction.17,18 Those who use this type of preventive therapy generally prescribe angiotensin converting enzyme inhibitors initially (88%), followed by statins, aspirin and angiotensin receptor blockers. Collaboration between metabolic units and cardiologists was considered necessary by 58% of those surveyed. Although this collaboration is not easy in practice, it at least demonstrates willingness to set up multidisciplinary hospital areas to improve the capitalization of health care resources.
Limitations of the Study
The response rate of 19% does not allow us to assert that the results reflect the opinion of all the cardiologists who are members of the Spanish Society of Cardiology, as those who responded were probably more interested in this particular subject. Notwithstanding this percentage, the results should not be rejected, as the opinions of persons interested in any topic are always useful. The percentages of the responses reflect a subjective opinion concerning the treatments evaluated or generally used, not those really prescribed. This explains the apparently inflated percentages of the use of certain drugs.
CONCLUSIONS
Those cardiologists who responded to the survey recognize certain shortcomings and needs in their knowledge of and attitude towards diabetes in their cardiac patients. The treatment given approaches that suggested in therapeutic guidelines. The deficiencies detected should motivate the setting up of educational initiatives, one of which is the creation of a specific working group.
Full English text available at: www.revespcardiol.org
ABBREVIATIONS
DM: diabetes mellitus.
Correspondence: Dr. J.L. Palma Gámiz.
Servicio de Cardiología. Hospital Universitario Ramón y Cajal.
Ctra. de Colmenar, km 9,100. 28036 Madrid. España.
E-mail: jlpalma@meditex.es