
To the Editor,
Infectious endocarditis (IE) is a microbial infection of the endocardium. It can be classified in acute, subacute and chronic, according to duration and clinical severity. Its characteristic lesion, the vegetation, is an aggregate of platelets, fibrin, microorganisms and inflammatory cells. The extension of the infection surrounding the valve annulus is a high mortality factor and frequently causes heart failure and the need for surgical treatment. Mycotic aneurysms can be a complication of infectious endocarditis. It is more frequently seen in the aortic root or the Valsalva sinus, where erosion can cause pericarditis, haemopericardium, heart tamponage or fistulas in the left or right heart chambers.1,2
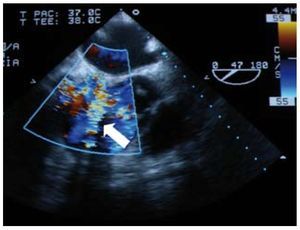
We present the case of a 47-year-old male, with a personal history of hiatus hernia and obesity, who was admitted with a dry cough, fever, asthenia, anorexia, and loss of weight of several months evolution. Previously he had consulted a physician due to a cough and poor general state of health and had been given antibiotic treatment with levofloxacin. However, as the symptoms persisted he came in to the emergency service at our hospital. Blood and urine analyses showed haemoglobin values of 10.8 g/dL, with normal blood differential, coagulation times, kidney and liver function, ions and urine sediment. Three blood cultures showed positive for Streptococcus viridans resistant to clindamycin, erythromycin and oxacillin. A transthoracic echocardiogram showed a moderately dilated left ventricle with preserved systolic function and an aortic tricuspid with vegetation and significant failure. A transoesophagic echocardiogram confirmed these findings and made it possible to see vegetation on the right coronary leaflet, impacting the ostium of the right coronary artery (RCA) during systole. This ostium was dilated and presented a continuation as a fistula with a continuous flow that drained the right atrium (RA) (Figure 1), at the outlet of which it was possible to see small mobile particles of vegetation. A thoracoabdominal CT with contrast was performed that showed small reactive and non-specific mediastinal adenopathies, well ventilated lung parenchyma with subpleural parenchymatous bands in both lower lobes, some with cavities ≤1cm, and suspected septic embolism (Figure 2); there were no significant findings in the remainder of the study. Antibiotic treatment was begun with G sodium penicillin and gentamycin, and the patient became afebrile. At no time were there signs of myocardial ischaemia, although there were symptoms of slight heart failure, which improved after deplective treatment. Before the patient underwent surgical treatment for chronic aortic endocarditis and suspected mycotic aneurysm at the origin of the RCA, in view of the complicated coronary fistula, a coronary angiography was performed, this showed dilation of the ostium of the RCA and a normal coronary anatomy. In an intervention with a heart-lung pump, the aortic valve was replaced by a mechanical St. Jude 23 mm prosthesis. It was found that the aortic valve had vegetation, a fistula and a mycotic aneurysm in the proximal part of the ostium of the RCA with the origin of the RCA within. Therefore, a pericardial patch was placed to occlude the aneurysm and a bypass of the RCA artery was performed with saphenous vein. No aortic periannular abscess was found. The immediate postoperative was favourable, and the patient is currently asymptomatic from the cardiovascular point of view.

Figure 1. Fistula with continuous flow draining into right atrium.

Figure 2. Subpleural bands of parenchyma in both lower lobes, some with cavities < 1cm.
Perivalvular extension is the most frequent cause of non-controlled infection in infectious endocarditis (IE) (including abscesses, aneurysms, pseudo-aneurysms, and fistulae).2 Mycotic aneurysms are an infrequent but not disdainable complication of IE. These are usually located in the aortic root, Valsalva sinus and visceral or cerebral arteries; but rarely in the coronary arteries, and are usually an autopsy finding.3,4