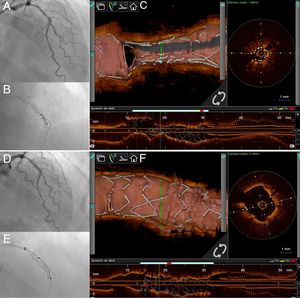
A 71-year-old man was admitted for acute coronary syndrome. Coronary angiography showed severe stenosis in the proximal anterior descending artery (video 1 of the supplementary data). Coronary angioplasty was performed by means of predilation with a noncompliant balloon and a cutting balloon. Subsequently, a 2.5 x 18 mm drug-eluting stent was implanted. After stent implantation, severe underexpansion of the distal third was observed, so postdilation was performed with noncompliant balloons at high pressure with no improvement (video 2 and video 3 of the supplementary data). Figure 1A shows the angiogram after postdilation of the stent, and Figure 1B the underexpanded stent visualized with StentBoost (Philips Medical Systems). Optical coherence tomography (OCT) showed the presence of heavily calcified circumferential plaque and severe underexpansion of the distal third of the stent (Figure 1C, video 4 of the supplementary data). With this outcome, it was decided to perform a coronary lithoplasty (Shockwave Medical, Fremont, California) expanding a 2.5 x 12 mm balloon at 4 atm and delivering 10 pulses of mechanical circumferential energy (video 5 of the supplementary data). Figure 1D shows the final angiographic outcome, while Figure 1E shows the correct expansion of the stent using the StentBoost tool. In addition, cracking of the calcified plaque, and correct stent expansion and apposition were assessed using OCT (Figure 1F, video 6 and video 7 of the supplementary data).

This case illustrates how the use of coronary lithoplasty may be of great assistance in the treatment of stent underexpansion.
Supplementary data associated with this article can be found in the online version, at https://doi.org/10.1016/j.rec.2019.04.009