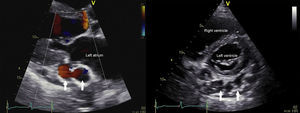
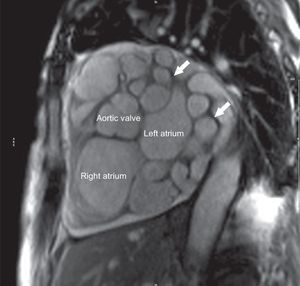
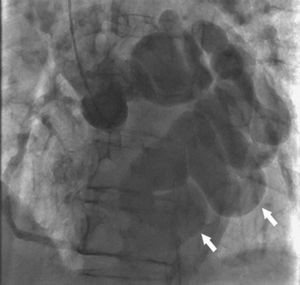
A nonagenarian man with previously excellent functional status presented with progressive dyspnoea and loss of appetite. Past medical history included well-controlled hypertension and atrial fibrillation. Clinical examination revealed right heart failure and a continuous murmur heard loudest at the left sternal edge. Transthoracic echocardiogram identified a basal posteroinferior vascular structure (Figure 1). Cardiovascular magnetic resonance in short axis view revealed extensive dilated vessel loops at the basal left ventricle, wrapping around the left atrium posteriorly and measuring 15-20mm in diameter (Figure 2). The right ventricle was moderately dilated with mild impairment and septal flattening consistent with volume-loading. Qp:Qs ratio of 2.1:1 indicated significant left-to-right shunt. Coronary angiography confirmed a large serpiginous arteriovenous fistula arising from the left coronary artery draining into the right atrium via coronary sinus (Figure 3, video of the supplementary material). Percutaneous closure was not deemed feasible. Surgical evaluation was declined, and the initial excellent response to diuresis was sustained at 6 months.



Coronary arteriovenous fistulas can be congenital or acquired, with an incidental prevalence on imaging of 0.9%. Acquired causes include atherosclerosis, arteritis, infection, malignancy, or trauma. In this case, given the absence of localising findings, potential etiologies include isolated congenital fistulae or atherosclerotic aneurysm. Coronary arteriovenous fistulas exhibit variable morphology and presentation with heart failure, endocarditis or angina from coronary steal phenomenon. For symptomatic individuals, therapies include percutaneous obliteration, embolization, or surgical closure; however, the optimal approach to small asymptomatic fistulae is less clear. This case provides novel insight into the natural history and extent of coronary arteriovenous fistula progression when discovered late in life.