To the Editor,
Iatrogenic dissection of the subclavian artery during cardiac catheterization is a subject that is seldom referred to in the literature, probably because of the low incidence and the possible existence of publication bias due to the fact that it concerns a complication.
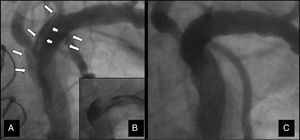
Our patient is a 75-year-old woman with hypercholesterolemia, hypertension, and a history of heart disease affecting the left main coronary artery and 3 coronary vessels. In 2002, she had undergone surgical treatment with triple bypass, from saphenous vein to obtuse marginal branch, saphenous vein to posterolateral branch of circumflex artery (left dominance), and left internal mammary artery to anterior descending artery. Asymptomatic from the cardiovascular point of view, she was admitted to the hospital in June 2010 due to prolonged angina at rest, with a high troponin level. She underwent coronary angiography via left radial artery, which revealed occlusion of proximal anterior descending, circumflex, and right coronary arteries, with patency of the grafts but severe lesion in the anastomosis between mammary coronary and anterior descending arteries. After consultation with the attending physician and the patient, the decision was made to perform a percutaneous interventional procedure in said lesion. The intervention was carried out via a left radial approach using a 6-Fr Judkins Right 4 guiding catheter. After balloon dilatation of the anastomotic stricture, during a follow-up injection we observed spiral dissection of the subclavian artery (Figure 1A) that affected the origins of the vertebral artery and the thyrocervical trunk, with contrast retention under vacuum conditions (Figure 1B). The patient reported mild pain in the left clavicular region, with no other symptoms. Angioplasty was completed by implantation of a drug-eluting stent within the anastomosis, with no additional complications. At the end of the procedure, we verified the persistence of the image showing the dissection, with no deterioration of the blood flow in the subclavian artery or in any of its branches. The absence of symptoms and the preservation of the blood flow led to the decision to initiate conservative medical management with dual antiplatelet therapy and other drugs for the treatment of the patient's ischemic heart disease and other diseases.

Figure 1. A: spiral dissection produced in the first procedure. B: image under vacuum. C: complete sealing 3 months later.
Three months later, the patient, who had remained asymptomatic until then, was readmitted because of a new episode of chest pain at rest, with no electrocardiographic or enzymatic changes. Coronary angiography was repeated and demonstrated the absence of restenosis or new coronary artery lesions and the disappearance of the evidence of dissection at the level of the subclavian artery and its branches (Figure 1C).
There are only 5 cases of iatrogenic subclavian artery dissection in the literature.1, 2, 3, 4, 5 In one of them, the authors reported the use of conservative management1 and did not perform angiographic follow-up to ensure the complete resolution of the complication. In the remainder, invasive approaches were employed. In all the published cases, the dissection occurred during catheterization of the mammary artery via femoral artery.
Catheterization of internal mammary artery in patients in whom this vessel has been employed as an arterial graft is a common practice in catheterization laboratories. Although catheterization is possible and safe using the femoral approach, this frequently cannot be achieved in a selective manner and requires more manipulation of the catheters than that necessary in native coronary arteries. Access via left radial or brachial artery has been proposed as a method to facilitate mammary artery catheterization, reducing the risk of damaging the subclavian artery.5 The left radial approach facilitates left mammary artery catheterization but, as illustrated by the case reported here, it does not avoid the possibility of subclavian artery dissection. In contrast to the published cases, in our patient the dissection was not accompanied by a deterioration of the blood flow. Since the radial approach was employed, the origin of the dissection (from distal to proximal) probably favored its lack of progression, its spontaneous sealing, and the success of its conservative management.
There is no solidly indicated treatment for an uncommon complication of this type. In those cases in which the blood flow is maintained and there are no signs of arterial ischemia or neurological distress, conservative management may be an effective strategy that avoids more serious complications.
Corresponding author: mlopezs@meditex.es