To the Editor,
The inflammatory pseudotumor is an expansile lesion characterized by an infiltrate of inflammatory cells and myofibroblasts, of unknown etiology, that affects lung tissue in children and young adults and very rarely in adults. The prognosis is usually favorable, since distant spread is uncommon. A number of cases of inflammatory pseudotumor of the heart have been reported in children and young adults, and only 15 cases in adults,1, 2, 3, 4, 5 in whom it is confined to the endocardium or to the valves.1 In adults, it has been described in any cavity, resembling myxoma or well-defined fibroelastoma, and it can generate a number of symptoms.4 Although treatment consists of excision of the tumor whenever possible,1 regression of the lesion with corticosteroid therapy has been reported in certain cases.6 Recurrence is not uncommon (13% to 37%), although the prognosis is usually favorable. There is a subtype of inflammatory pseudotumor, the calcifying lesion, which could correspond to a more advanced stage in the evolution of the inflammatory pseudotumor, with abundant collagen fibers, dystrophic calcifications,2 and a characteristic immunohistochemical pattern (positivity for muscle-specific actin, FXIIIa, CD68 and vimentin and negativity for CD34). Although the inflammatory pseudotumor can occasionally exhibit mitosis, the absence of atypia differentiates it from a true sarcoma.3 In the literature, we have found no descriptions of primary calcifying inflammatory pseudotumor of the heart in adults, and only two cases in children,2, 7 nor has transmural involvement been reported to date.
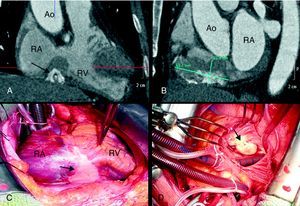
Our patient, a 57-year-old nonsmoker, presented with progressive angina. The results of physical examination and the electrocardiogram were normal. Coronary angiography revealed 95% stenosis in the circumflex artery, which was treated by metallic stent placement, and proximal right coronary artery occlusion. We identified a calcified mass adjacent to the diaphragm, with extrinsic compression of right coronary artery. Transthoracic and transesophageal echocardiography showed dilation of right atrium and a large calcified mass in the posterior region of the atrioventricular groove, with protrusion into right annulus and transtricuspid gradient. Cardiac magnetic resonance revealed heterogeneous contrast medium uptake, which indicated vascularization and signs of a high fibrous content. Multislice computed tomography disclosed a large, poorly defined, calcified mass (63.7mm×22.9mm) infiltrating the groove (Figure 1A and B). There was no evidence of hypermetabolism or metastasis in positron emission tomography. Once informed consent had been obtained, surgery was performed with diagnostic and therapeutic intent. Following sternotomy, we identified a large calcification in anterior pericardium (Figure 1C), the lateral and inferior walls of right atrium and the atrioventricular groove, with inclusion of right coronary artery and transmural infiltration of the base of both ventricles, protruding 4cm toward the interior of the tricuspid ring (Figure 1D). The perioperative histological analysis revealed the presence of an inflammatory infiltrate with no evidence of malignancy. The mass was partially resected and reconstruction of the groove with bovine pericardium and implantation of a tricuspid bioprosthesis were required. As a consequence of the surgery, a permanent pacemaker was implanted due to complete atrioventricular block. The subsequent histopathological analysis identified an inflammatory infiltrate composed of lymphocytes, plasma cells and occasional mesenchymal cells, without mitosis (Figure 2A-C), and areas of collagen with secondary calcifications (psammoma bodies) (Figure 2A). The immunohistochemical study demonstrated positivity for muscle-specific actin, CD68, CD4 (Figure 2D and E) and CD8, and negativity for desmin, S100 protein and CD34, all findings compatible with the diagnosis of calcifying inflammatory pseudotumor. After 2years of follow-up, the patient is asymptomatic and shows no evidence of recurrence or progression of the tumor.

Figure 1. A and B: tomographic images of the calcified mass in the atrioventricular groove. C: an aspect of the calcification of the pseudotumor during surgery (arrow). D: protrusion of the lesion into tricuspid annulus (arrow). Ao, aorta; RA, right atrium; RV, right ventricle.

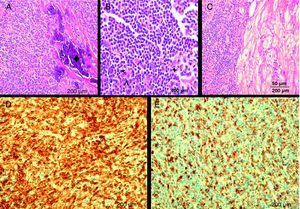
Figure 2. Histological images. A-C: hematoxylin and eosin staining with infiltration by mature lymphocytes (*), histiocytes (arrowhead), plasma cells (+), and calcification (♦) in myocardium. D: CD4+ cells (T lymphocytes). E: CD68+ cells (histiocytes). Scale bar=50μm.
Corresponding author: e.zamora@telefonica.net