To the Editor,
We present the case of a 91-year-old patient with no known cardiovascular risk factors who came to the emergency room for sudden onset of dyspnea, chest pain, and hypotension. A few days prior, he had a respiratory tract infection that was treated with antibiotics.
Upon arrival to the emergency department, baseline oxygen saturation was 91% and arterial pressure 98/68mmHg; hypoxemia and hypocapnia were documented on arterial blood gas measurement. Pulmonary thromboembolism was suspected, but emergency computed tomography (CT) angiography ruled out this diagnosis. Cardiorespiratory auscultation revealed rhythmic tones, with a grade 3/6 apical pansystolic murmur, radiating toward the axilla. The patient presented a decreased bilateral vesicular murmur with bibasal crackles, and edema of the lower limbs. The electrocardiogram showed sinus rhythm with left axis deviation and lack of R wave progression in the precordial leads. A slightly enlarged heart and mild bilateral pleural effusion were visualized on chest radiography.
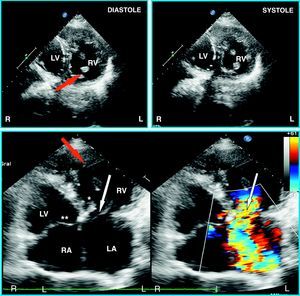
Doppler echocardiography, performed to investigate suspected heart failure, showed several relevant findings (Figure 1). The heart was located on the left side. The morphologic left atrium (LA) was at the left and received flow from the pulmonary veins, and the morphologic right atrium (RA) received flow from the caval veins. The LA connected with an anatomic right ventricle; the connection was achieved through an atrioventricular (AV) valve that had three leaflets (tricuspid) and presented a prolapse with eversion of one of the leaflets due to rupture of the tendinous cords. The ventricle located to the left (systemic) connected with a non-bifurcated vessel (aorta), situated to the left and anterior to the bifurcated vessel (pulmonary artery [PA]). These findings indicated a diagnosis of congenitally corrected transposition of the great arteries (CCTGA) with failure of the systemic AV valve. Based on this suspected diagnosis, we reviewed the CT angiography study and recognized these unusual findings (Figure 2).

Figure 1. Doppler echocardiography showing an anatomic right ventricle located to the left. Note the greater trabeculation and hypertrophy than in the anatomic left ventricle, the presence of a moderating band (red arrow), and the more apical implantation of the septum valve of the systemic atrioventricular valve (*) in comparison to the anatomic left atrioventricular, located at the right in this case (**). The systemic atrioventricular valve presents eversion of one of the leaflets (white arrow), which originates a severe insufficiency jet. LA, left atrium; LV, anatomic left ventricle; RA, right atrium; RV, anatomic right ventricle.

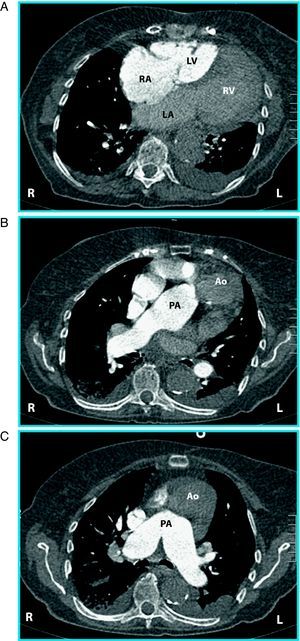
Figure 2. Computed tomography angiography angiography with sequential axial slices of the heart and great vessels following intravenous contrast injection. In A and B, the ascending aorta is seen to arise in a position anterior and to the left of the pulmonary artery origin, which is in a posterior and right position. In B and C, the aorta is seen to arise from an anatomic right ventricle, which is located at the left. Ao, ascending aorta; LA, left atrium; LV, anatomic left ventricle; PA, pulmonary artery; RA, right atrium; RV, anatomic right ventricle.
CCTGA is a rare cardiac malformation, consisting of AV and ventriculoatrial discordance: The RA is connected to the morphologic left ventricle, which gives rise to the PA, whereas the LA is connected to the morphologic right ventricle, which gives rise to the aorta. The aorta is usually, but not always, positioned anterior and to the left of the PA, and the great vessels tend to be parallel, instead of crossing. This condition can be associated with other cardiac defects, the most common being Ebstein anomaly and ventricular shunt (in the presence or absence of pulmonary, valvular, or subvalvular stenosis). The presence of persistent ductus arteriosus is less common.1, 2, 3
The prognosis depends on the associated lesions. The most common is failure of the left AV valve (anatomic tricuspid), either because it is an Ebstein-like valve or because of functional valve failure due to dilatation of the systemic ventricle. Tendinous cord rupture, as occurred in the case presented, is an infrequent trigger of heart failure. If there are no concomitant lesions, the patient can remain asymptomatic even up to the seventh or eighth decade of life.
Corresponding author: mircardjla@gmail.com