To the Editor:
Catheter ablation has become the treatment of choice for symptomatic patients with accessory pathways (acP) that connect the atria and the ventricles. For the most part, these connected both cardiac chambers at the level of the atrial-ventricular rings, although occasionally they are located at a certain distance from these, in unexpected places and generally unexplored.
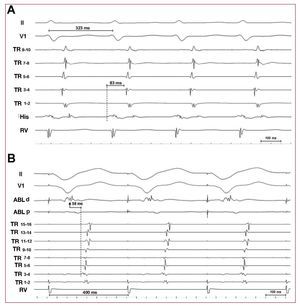
We present the case of a 34-year-old male with no structural cardiopathy, referred for an electrophysiological study due to a history of several years' evolution of paroxysmal supraventricular tachycardia. The baseline ECG was normal. The study was carried out with 3 tetrapolar catheters for the His region, the right ventricle and the right atrium. The existence of ventricular pre-excitation was excluded. Ventricular stimulation revealed ventricular-atrial (VA) conduction, eccentric and not decremental, with earlier atrial activity in the high right, which indicated a concealed right acP. A multielectrode "deflectable" catheter was placed in the right atrium, to aid in the cartography of activation of the tricuspid ring (TR) and to localised the atrial insertion of the acP with greater precision, and it was observed that the earlier atrial activation was registered in the TR lateral position (bipole 3-4). In a highly reproducible manner, an orthodromic tachycardia was induced (Figure 1A), with a cycle lenght of 323 ms, a septal AV interval of 106 ms and in lateral TR of 83 ms, with an atrial activation sequence identical to that obtained in sinus rhythm with ventricular stimulation. The active participation of the right acP in the orthodromic tachycardia was confirmed with tachycardia stimulation manoeuvres. For the ablation, a "deflectable" tetra-polar catheter 7 Fr (Marin® 4 mm, Medtronic) was used, advancing through a preformed introducer (Fast-Cath SR3®, St. Jude Medical). During continued ventricular stimulation, 9 failed radio frequency applications were carried out (10-25 s; 60°; 55W) in the TR lateral position, where earliest results were obtained with respect to the earliest atriogram (TR 3-4), while never over 10 ms and without local AV continuity. Faced with these findings and the observation of great concomitance of atrial activation in the electrode pairs of the TR catheter, we decided to map the right atrial appendage (Figure 2), in the baseline, precocities over 50 ms and local VA continuity were found, without observing any acP potential (Figure 1B). Five application were carried out in this region, the last of which (120 s; 50º; 30 W) managed to eliminate the acP conduction to 10 s permanently and without complications.

Figure 1. A: electrocardiographic derivations (II and V1) and intracavity registers of activation in the tricuspid ring (TR) (1-2 are the distal pair), His and right ventricle (RV) of the tachycardia. B: registers in the acP ablation point during continued stimulation from RV. ABL d, p: ablation catheter, pair of distal and proximal electrodes.

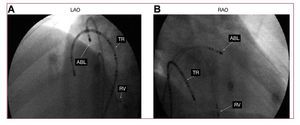
Figure 2.A: x-ray projection left anterior oblique (LAO) in the point of acP ablation. B: x-ray projection right anterior oblique (RAO) in the point of acP ablation. ABL, ablation catheter; TR, catheter for tricuspid ring mapping; RV, right ventricle catheter.
The acP with atrial insertion in the atrial appendage is due to epicardiac connections between this and the adjacent ventricle, whether congenital or surgically created.1,2 The norm is, as occurred in this case, the absence of an acP potential in the ablation exit point, due to the fact that these pathways are a consequence of a direct connection between the atrial appendage and the ventricular myocardium. Ablation from the right atrial appendage usually requires its isolation with the applications of the atrial appendage that joins the ventricle, which usually obliges to use numerous applications.3 It could be necessary on occasion to use irrigated tip catheters due to the limited blood flow in the interface between the catheter and the atrial appendage trabeculated surface, or an epicardial, surgical or percutaneous approach.1,4