To the Editor:
The treatment for cardiac wounds due to pellets from firearms is still controversial because of the limited number of cases analyzed at each hospital, and the enormous variation in the location of intracardiac pellets and the symptoms they produce. The therapeutic options for this entity include conservative treatment, pericardial drainage, and surgical removal of the shotgun pellet, although each patient's treatment should be individualized. We describe an adult with a firearm-related cardiac wound in which a shotgun pellet became lodged in the interventricular septum and was successfully treated using a conservative approach.
A 37-year-old man consulted at our hospital for a hunting accident in which he was wounded with a firearm from an approximate distance of 20 m. At arrival, the patient was conscious, hemodynamically stable, and with good oxygen saturation. The physical examination revealed multiple wounds 0.5 cm in diameter caused by shotgun pellets in the legs, arms, abdomen, and anterolateral region of the left thorax. There were no signs of heart or respiratory failure.
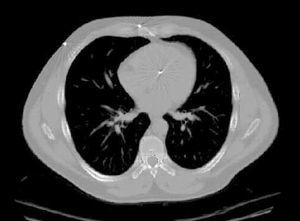
The electrocardiogram showed sinus rhythm with no other alterations; the chest x-ray detected multiple substernal and bilateral intrathoracic shotgun pellets associated with a left pneumothorax that required percutaneous drainage. The echocardiogram detected moderate pericardial effusion (1 cm maximum separation between the layers) and the presence of a shotgun pellet in the muscle portion of the interventricular septum, near the left ventricular outflow tract. There was no ventricular septal defect, and the contractility of both ventricles was normal. Computed tomography (CT) confirmed the presence of the foreign body embedded in the interventricular septum (Figure). In addition, a laparoscopic abdominal examination ruled out intraperitoneal visceral lesions.

Figure. Chest computed tomography shows a shotgun pellet lodged in the muscle portion of the interventricular septum.
Because there were no arrhythmias and no signs or symptoms of heart failure, conservative treatment was undertaken. Hemodynamic and respiration variables remained stable, with no cardiovascular symptoms throughout hospitalization. The patient was discharged at 7 days. At 1 year, there was no increase in pericardial effusion and he was completely asymptomatic. On follow-up CT, the shotgun pellet was surrounded by fibrous tissue in the myocardial wall of the interventricular septum.
Cardiac wounds due to shotgun pellets are considered an extremely rare entity, for which there is no standard treatment protocol due to their low incidence in our clinical practice.1,2 These pellets are small projectiles that may remain partially or totally embedded in the myocardium or pericardium, or free in the cardiac cavities, or the pericardial space. The associated clinical manifestations may be heart failure, tamponade, arrhythmias, pericarditis, or embolic phenomena,3,4 depending on the number and location of the projectiles. However, shotgun pellets in the myocardium can also be clinically and hemodynamically well-tolerated.
The case we describe is the only wound in the interventricular septum due to a shotgun pellet not removed by surgery that has been published in Spain and 1 of the first in the English scientific literature. In a recent review, Symbas et al5 found a single case of shotgun pellet in the interventricular septum that had been removed, from among 222 cardiac projectiles reported. Other foreign bodies found at this site included 2 bullets and 2 blades that were not removed, possibly because the potential risk was greater than the potential benefit of surgery.
The treatment of heart wounds due to shotgun pellet should be individualized.6 The success of conservative treatment in this case supports the concept that projectiles located in the interventricular septum may be well-tolerated and only require monitoring, provided that the patient remains asymptomatic and hemodynamically stable. Surgical examination and excision should be considered with the onset of arrhythmias, heart failure, ventricular septal defect, or cardiac tamponade.