To the Editor:
Drug-eluting stents (DES) have led to considerable changes in interventional cardiology. Registries and randomized studies have shown that these stents provide clinical benefit, mainly by decreasing the incidence of restenosis.1 However, indiscriminate use of these devices has been questioned.2
Complications, such as acute and subacute thrombosis,3 inadequate late apposition phenomena, and coronary aneurysms (CA) at the implantation site, have been reported with DES.4
We describe a 67-year-old patient diagnosed with a CA in the left anterior descending (LAD) artery and the right coronary artery (RCA) 4 years after implantation of a DES (Cypher®).
The patient had a personal history of dyslipidemia and hypertension, and a family history of ischemic heart disease. After presenting a non-Q wave myocardial infarction in 2002, he was treated for 2 significant lesions in the LAD and RCA. In the LAD, angioplasty with a 2-mm balloon was performed and a 2.75x18-mm Cypher stent was implanted. A 2.5-mm balloon was used in the RCA and a 3.0x18-mm Cypher stent was implanted, with excellent angiographic results. Abciximab was used and clopidogrel was added to the patient's therapy, which was maintained during follow-up.
In June 2006 he was admitted for angioedema of the lip and tongue (related to angiotensin-converting enzyme inhibitor therapy). The patient reported clinical symptoms of recurrent angina with the first effort of the day during the last month.
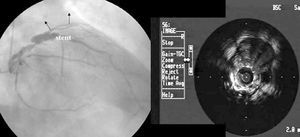
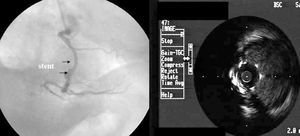
Coronary angiography showed a 50% distal lesion in the left main coronary artery, 70% stenosis in the LAD proximal to the stent, and irregular aneurysmal dilation over the entire length of the stent with a maximum angiographic diameter of 9 mm. An irregular aneurysmal dilation was observed in the RCA in the stent area, which extended over its entire length and had a maximum diameter of 8 mm; an 80% lesion was also visualized in the origin of a posterolateral branch. In both arteries, areas of aneurysmal dilation were observed only in the stent sections.
The expansion and symmetry of both stents was corroborated by intravascular ultrasound with a large, echo-free area and with abnormal apposition, and aneurysmal dilation in both coronaries. In the LAD, the stent was 2.8 mm in diameter, partial neointimal proliferation was evident, and the area was 6.8 mm2. The aneurysm was highly irregular and had a maximum diameter of 9.1 mm, and an area of 46 mm2, with an image indicative of flow through the metal parts. Similar findings were observed in the RCA: proper stent expansion and symmetry (diameter of 3.1 mm, area of 7.1 mm2), plus abnormal apposition, and irregular aneurysmal dilation over the entire course of the vessel, with a diameter of 8 mm and an area of 45 mm2 (Figures 1 and 2).

Figure 1. Left coronary: angiography and intravascular ultrasound of the left anterior descending artery.

Figure 2. Right coronary: angiography and intravascular ultrasound.
Coronary artery bypass surgery was indicated, confirming aneurysms at the retropulmonary area of the LAD stent and at the RCA stent. Left mammary grafts were placed to the LAD, and saphenous grafts to the obtuse marginal artery, and the posterior descending artery. The postoperative progress was unremarkable.
Coronary aneurysms, which may have several pathophysiological mechanisms, are uncommon and their clinical evolution is poorly understood. The treatment and potential complications of these aneurysms are uncertain. They have been related to coronary arteriosclerosis, and can also appear after an interventional procedure.5
Early and late onset CAs have been reported in the DES implant area. Early cases in both sirolimus and paclitaxel DES have been related to inflammation and infections,6 whereas in late cases, the mechanisms involved can be complex. Evidence of inflammation related to the drug, polymer, or metal has been described, as well as persistent inflammatory phenomena, with a delay in endothelialization of the stent area in tissues exposed to polymer or drug.4
Aneurysms have been described in 2 coronaries implanted with sirolimus-eluting stents, leading to speculation on possible hypersensitivity to the drug, although the pathophysiological mechanism causing the dilation has not been determined precisely.7
The lack of physiopathological and prognostic information, the natural course of the condition, and the potential complications of CAs hinder the therapeutic decision. In our case, the coexistence of significant lesions in the left main stem facilitated the surgical decision.
Long-term clinical follow-up of patients with DES and in-depth clinical and experimental studies on the possible chronic inflammatory processes are needed. Patients with hypersensitivity to the stent components, polymer, or drug coating, should be identified in order to decide on possible prevention and treatment.