
To the Editor,
Endovascular repair (EVR) of infrarenal abdominal aortic or descending thoracic aortic aneurysms is widely described in recent literature.1,2 Unfavourable anatomical conditions such as visceral branch disorders limit the application of EVR. However, new technologies provide for endovascular treatment in experienced centres.3
We report the case of a 79-year-old male, former smoker with a history of hypertension, Parkinson's disease and hostile abdomen secondary to left hemicolectomy for a colorectal carcinoma performed one year before admission. Following the completion of a follow-up computed tomography (CT) for his neoplastic disease, a type II thoracoabdominal aortic aneurysm (TAAA) was found with a maximum diameter of 65 mm at the abdominal level, 53 mm at the renal artery outlet level and 42 mm from the celiac trunk to 5 cm distal to the outlet of the left subclavian artery. Given the high comorbidity and the risk of open surgery, we opted for endovascular treatment despite the anatomical complexity. A customised modular endoprosthesis with visceral branches that would exclude the entire TAAA was designed for this procedure (Zenith Cook®, Medical Inc., Bloomington, Indiana, United States).
Surgery was performed with general anaesthesia in the endovascular operating room. In order to protect the spinal cord and maintain pressures ≤10 mm Hg, we placed a spinal catheter for cerebrospinal fluid (CSF) drainage at the L4-L5 level for 48 hours. Mean arterial pressure (MAP) was maintained at >90 mm Hg (periprocedure).
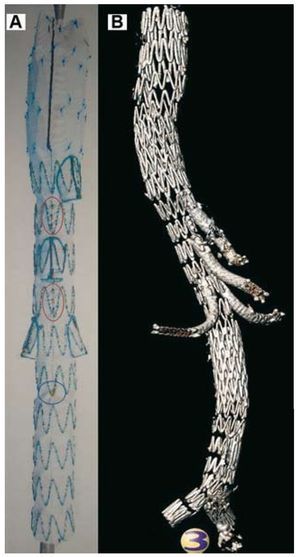
From a right femoral surgical approach, a tapered thoracic component was implanted (44´30´143 mm), followed by the thoracoabdominal component (Figure 1) with visceral branches (quadruple ramification, 32´22´239mm, for the celiac trunk, superior mesenteric and renal arteries) and by the abdominal bifurcated endoprosthesis (24´20´171 mm). The left femoral artery was used to insert the contralateral iliac branch (12´20´73 mm). From a left axillary surgical approach, the four visceral shunts were completed using PTFE-covered stents (Fluency® Plus, Bard, Tempe, Arizona), reinforced with bare Luminexx® stents (Bard) to avoid angulation.

Figure 1. Customised branched thoracoabdominal graft. A: segment that makes up the 4 visceral branches. B: postoperative 3-dimensional reconstruction of all components.
The procedure was successfully completed in four hours, 30 minutes. A I-II/V monoparesis of the right lower extremity was detected on the first postoperative day, which evolved favourably with an increase in MAP and CSF drainage. CT angiography performed on the fifth day confirmed the absence of endoleaks and the permeability of all visceral branches (Figure 2). The patient was discharged on the seventh postoperative day after receiving rehabilitation therapy.

Figure 2. Computed CT angiography with 3-dimensional reconstruction on the fifth postoperative day, which shows the permeability of all visceral branches. A: frontal view. B: left lateral view.
This case demonstrates the feasibility of performing a complete EVR of a complex TAAA using tailored branched endoprostheses. Furthermore, except for specific centres of excellence,4 this therapeutic approach offers lower morbidity, mortality and paraplegia rates than conventional open surgery.5 However, broad experience with EVR of complex aortic aneurysms is recommended prior to implementing this new technique. To date there are still very few centres that are building up positive experiences.6,7
We believe that in the future this will be the technique of choice in managing complex aortic diseases. As a result, we believe that this is a feasible procedure that can offer an effective alternative to the vast majority of patients with TAAA, especially those whose characteristics make them ineligible for conventional open surgery.