
We present the case of a 66-year-old patient suffering from obesity, hypertension, and dyslipidaemia who was admitted to the heart surgery department of our institute on October 28, 2009, with a diagnosis of severe aortic stenosis and coronary heart disease. These diagnoses had been established 11 months before due to the incidental finding of a heart murmur while performing transthoracic and transoesophageal echocardiograms. The diagnosis was severe aortic stenosis (aortic valve peak gradient of 68, average of 46 and 0.95 cm2 area) with preserved systolic function and left ventricular concentric hypertrophy (15 mm intraventricular septum and 14 mm posterior wall). Cardiac catheterisation showed coronary artery disease (80% occlusive lesion in the proximal third of the anterior descending artery and 75% in the middle third of the circumflex artery). At the time of surgery, we did not suspect alkaptonuria in our patient, but the surgical findings revealed partial fusion and calcification of the aortic valve flaps. Also, blackish pigmentation of the aorta and the coronary arteries was observed (Figure 1). We proceeded to replace the valve with a number 21 mechanical prosthesis and two bypass aortocoronaries (left internal mammary artery to descending artery and internal saphenous vein to the marginal one).

Figure 1. Internal black discoloration of the aorta and scleral pigmentation of the right eye.
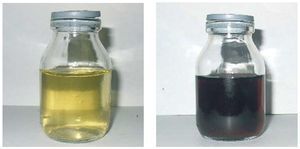
Given this unusual finding, we researched the possible causes and conducted a more thorough case history review. The patient said he had had arthralgia in the shoulders, spine, hips and knees for the past 20 years. A physical examination showed stiffness and crepitus on the shoulders, hips and knees as well as blackish pigmentation in the sclerae (Figure 1). X-rays of the spine, shoulders and hips revealed lumbar spondyloarthrosis, coxarthrosis, gonarthrosis, and shoulder osteoarthritis. The patient's urine was collected, which turned blackish after 24 hours of contact with light and the environment, a common occurence with alkaptonuria (Figure 2). Furthermore, homogentisic acid was detected in the urine. Lastly, a histological study of the aortic flaps showed hyaline degeneration, fibrosis, calcification and dark brown pigmentation of the edges of the valves.

Figure 2. Patient's urine changed colour after 24 hours of exposure to the environment.
Alkaptonuria is a rare disease that is transmitted with an autosomal recessive pattern, with a frequency of 1 case per 200 000 inhabitants. It is a tyrosine metabolism disorder in which homogentisic acid oxidase deficiency causes the excretion of large quantities of this acid in the urine and the accumulation of its oxidised pigment in the connective tissues (a disorder known as ochronosis).1,2 This disease can go unnoticed until adulthood when patients exhibit joint disorders (pain, stiffness and limited movement of hips, knees, and shoulders), patches of grey-brown scleral pigment and overall darkening of the ear. Apart from these disorders, pigmentation can occur in the heart valves, larynx, tympanic membranes and skin. Some patients also develop kidney or prostate stones.1-4
Although we did not find any study in our literature search that related aortic stenosis or coronary heart disease with alkaptonuria, various cases have been published in which these conditions occurred in the same patient.3-6
The association between alkaptonuria and aortic valve disease has been postulated and it has also been reported that this valve is the most affected by this condition, followed by the mitral and the pulmonary valves. Aortic stenosis is the most commonly associated disease, although it has also been linked to aortic and mitral regurgitation.4 Furthermore, cases like ours have been published linking alkaptonuria with coronary artery disease.5
Electron microscopy studies of a patient with alkaptonuria and aortic stenosis showed changes consistent with valve cell death associated with homogentisic acid deposition. The authors concluded that the intracellular deposit of pigment caused the death of these cells and probably produced dystrophic calcification with consequent valvular stenosis.6