To the Editor,
Aggressive angiomyxoma is a rare mesenchymal neoplasm of the soft parts of the pelvis. It is a benign lesion with a high incidence of recurrence that presents mainly in women in the third or fourth decades of life, and particularly affects the pelvis and perineum.1 The cell of origin is the myofibroblast.2
We describe a 38-year-old woman with a tumor of this type and a mass in the right cardiac chambers on imaging study. Following surgery, this was shown to be part of the tumor growth that had reached the right atrium through the inferior vena cava.
The patient consulted for abdominal swelling of several months' evolution that was associated with abdominal and lumbar pain, as well as a feeling of dysthermia and vomiting. An abdominal mass was palpated in the emergency room. Abdominal sonography and computed tomography (CT) revealed a heterogeneous solid mass (37±27±17 cm) occupying the abdominal and pelvic cavity, with an uncertain origin. The images were consistent with a "venous thrombus" that occupied the lumen of the inferior vena cava along its entire length, the left renal vein, and the common iliac veins, extending to the right cardiac cavities.
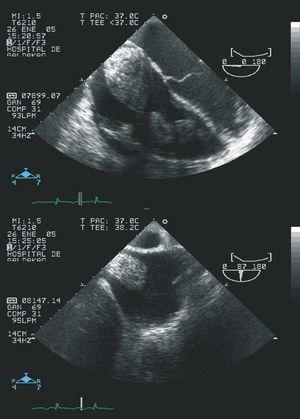
Transthoracic and transesophageal echocardiography showed a huge mass in the right atrium that prolapsed into the right ventricle through the tricuspid valve, without reaching the pulmonary artery. The transesophageal study indicated that the mass was not related to the interatrial septum, but entered through the inferior vena cava. In view of the possibility that the mass was a large venous thrombus, anticoagulant therapy was initiated (Figure 1).

Figure 1. Transesophageal imaging showing a large mass in the right chambers that penetrates from the inferior vena cava.
The mass was biopsied using a lumbar approach and showed a lax myxoid-like stroma, with an accompanying vascular pattern and minimal disperse mesenchymal cellularity without atypia. Immunohistochemistry was positive for desmin and actin in the vascular and stromal component, but S-100 techniques were negative and CD 34 was positive only in the vascular component.2-4 The stromal cells showed nuclear positivity for progesterone and estrogen; the series of results was consistent with aggressive angiomyxoma of the pelvis.
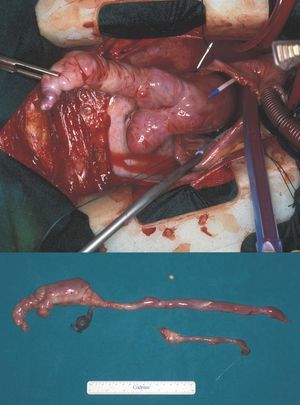
Based on these findings, a decision was made to first remove the large cardiac mass. Surgery was undertaken, revealing that the cardiac mass was not a thrombus, but rather part of the abdominal tumor, which had grown to occupy the inferior vena cava segment and had reached the right atrium (Figure 2).

Figure 2. Tumor resection during cardiac surgery. Macroscopic specimen.
The abdominal mass was resected en bloc in a second procedure. The histologic study showed an aggressive angiomyxoma, with a diameter of 36 cm, affecting the uterus and both fallopian tubes. Complete removal of the tumor was not possible. The postoperative course was good and the patient was discharged home 13 days after the abdominal surgery.
One year after surgery, the patient remained asymptomatic despite local recurrence of the mass in the abdominal area. Given the benign nature of the tumor and the difficulty of removal, it was decided to perform follow-up with periodic monitoring by abdominal CT.
The interest of this case lies in the unusual extension to the cardiac cavities, the first such case reported in the medical literature. Only one other case involving pulmonary and mediastinal metastases has been described. In our patient, cardiac involvement does not appear to have occurred by remote tumor implants, but rather by invasion of the inferior vena cava and progression toward the cardiac cavities.4,5