To the Editor,
Kawasaki disease (KD) is a systemic vasculitis of unknown etiology that can produce coronary artery aneurysms in up to 25% of untreated cases. The disease presents mainly in young children and is rare in adulthood.1
We describe a 28-year-old man, a smoker of 4 cigarettes a day as the only cardiovascular risk factor. The only pathological history of interest was hospitalization 6 months earlier for fever of one month's duration, accompanied by generalized erythema and musculoskeletal pain. Following various examinations and blood tests that revealed thrombocytosis, hypoalbuminemia, an abnormal liver profile, and elevated erythrocyte sedimentation rate and C-reactive protein, the patient was discharged with a diagnosis of fever of unknown origin. Six months later he was readmitted for exertional angina. Coronary angiography showed severe diffuse disease of the entire coronary vasculature (Figures 1 and 2). The clinical symptoms and findings of the additional examinations led to a diagnosis of KD that had gone undiagnosed in the acute phase (6 months previously). Treatment with aspirin, acenocoumarol, and an antianginal drug was started. The patient was discharged and after 2 months' follow-up, presented stable exertional angina in functional class I.

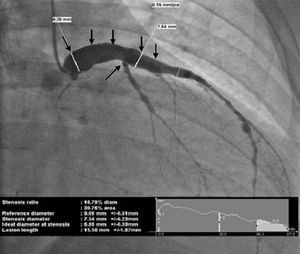
Figure 1. Coronary angiography; right anterior oblique view showing a giant aneurysm (9 mm in diameter) of the left main coronary artery and the proximal left anterior descending artery, affecting the origin of the first septal and first diagonal (arrows), with occlusion of the proximal circumflex and severe diffuse disease of the distal vessel.

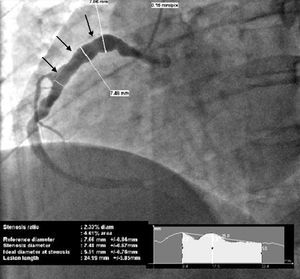
Figure 2. Coronary angiography; left anterior oblique view depicting a dominant right coronary, with aneurysm of the proximal and middle segments, approximately 7 mm in diameter (arrows), and severe diffuse disease of the distal vessel.
The classic diagnosis of KD is based on the presence of fever lasting 5 or more days and 4 or more of the following clinical signs: cutaneous alterations in the limbs, polymorphic rash, nonexudative bilateral conjunctivitis, involvement of the lips and oral cavity, and cervical adenopathies. In patients with fever lasting 5 or more days that meet fewer than four of the above clinical signs, the diagnosis can be made if coronary disease is detected, usually by 2D echocardiography or angiography.1 Multislice computed tomography has recently been described as a useful technique to detect coronary aneurysms in KD, particularly in patients with a poor echocardiographic window (as tends to occur in adults) and no clear indication for invasive studies, although this does not specifically correspond to the case we describe.2 Coronary dilation or ectasia is defined as an inner vessel diameter ≥2 SD above the age- and body surface-adjusted mean, but <4 mm. Aneurysm3 is defined as a diameter ≥4 mm and <8 mm, and giant aneurysm as a diameter ≥8 mm.
The onset of KD in adulthood is extremely rare and, to our knowledge, only 63 cases have been published to date. Several cases of myocardial infarction attributed to KD undiagnosed in childhood have been reported in young adults, one of them published in the Revista Española De Cardiología.4 The case we present is the first clinical case of KD of adult onset with coronary involvement described in the Spanish medical literature.
In children, diagnosis and early immunoglobulin treatment is associated with a lower incidence of coronary aneurysms and therefore, with lower morbidity and mortality.1,5 Although KD is a rare entity in adults, it should be considered in the differential diagnosis of febrile syndrome with skin rash, because early diagnosis and treatment is also likely to decrease the incidence of coronary involvement, as well as morbidity and mortality in adults.