To the Editor:
Coronary aneurysms are uncommon events. They occur most frequently in the right coronary branch, and the most common aetiology is arteriosclerotic disease. Other causes are external damage, inflammatory and connective tissue disease, infectious diseases, and congenital aneurysms.1-3
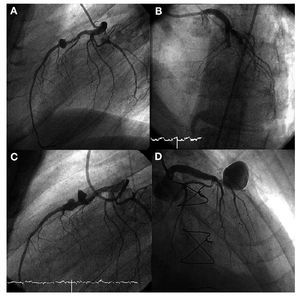
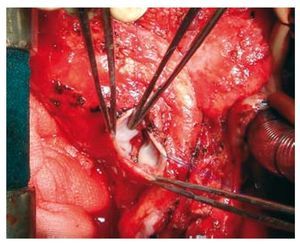
We present the case of a 60-year-old male, a current smoker with diabetes and high cholesterol. He had been admitted 1 year before with a pneumococcal bacterial infection of unknown origin that was treated with ceftriaxone. The patient came to the emergency room with pericardial thoracic pain, and had experienced cold symptoms and fever over the past few days. The ECG showed no signs of acute pericarditis, and QS was in V1 and V2. Laboratory analyses showed isolated elevation of troponin T. The echocardiogram showed mild anterior hypokinesia, with a conserved ejection fraction and a minimal pericardial stroke. Due to suspected anterior infarction, we ran a coronariography (Figure 1A). The middle descending anterior artery presented a moderate arteriosclerotic lesion and, directly distal, a saccular aneurysm 10 mm in diameter. Anti-inflammatory treatment was administered and the patient remained asymptomatic at the site. In light of the coronariography findings and with a clinical suspicion of myopericarditis, we performed a stress test with technetium in order to clinically evaluate the lesion in the anterior descending artery. The patient began experiencing chest pain and general discomfort at 6 minutes of exercise, and the electrocardiography recorded an ST segment increase. The patient was transferred to the haemodynamics lab, where total occlusion was observed at the level of the middle anterior descending artery, before the aneurysm, (Figure 1B); an angioplasty was performed and 2 conventional stents implanted. After reperfusion, we observed that the aneurysm had doubled in size (Figure 1C). In the days that followed, the patient developed right congestive heart failure and output failure. In a series of echocardiograms, we observed increasing pericardial effusion, and in light of a suspected burst aneurysm, we opted for an emergency surgical procedure. The aneurysm was still intact, the pericardium was 2 cm thick and the pericardial fluid was purulent. All signs indicated an infectious disease, which involved a risk of superinfection at that location in the event of resection of the aneurysm and derivation through a mammary artery. A bilateral antephrenic pericardiectomy was performed and samples were taken for culturing which revealed Streptococcus pneumoniae. After completing a 6-month antibiotic treatment with ceftriaxone, a new coronariography was taken which showed that the aneurysm had increased in size (Figure 1D). Faced with a risk of complications (thrombosis, embolism, rupture) we decided to perform another surgical procedure involving aneurysm resection and derivation of the internal mammary artery to the anterior descending artery (Figure 2). The microbiology culture was sterile and the histological study showed non-specific fibrosis. The patient underwent the operation with no complications and was discharged after 4 months of hospitalisation. One year later, he remains asymptomatic.

Figure 1. A: saccular aneurysm 10 mm in diameter halfway down the left anterior descending artery. B: acute occlusion in the middle area of the anterior descending artery before aneurysm. C: after opening the vessel, verification that the aneurysm had doubled in size. D: last coronariography, which revealed a giant aneurysm with a high risk of complications.

Figure 2. Aneurysm resection surgery. Significant fibrosis and inflammation in the interior. The previously implanted stent can be seen in the background.
The natural history and treatment steps are not well defined for arteriosclerotic coronary aneurysms, but they are related to the size and symptoms. Some authors consider that a size >1 cm or 3-4 times the size of the native vessel is an indication for surgery4 or for percutaneous closure by implanting a stent graft. Other authors believe that if the aneurysm is small and does not present severe lesions or complications, the long-term prognosis is good and it can be handled with medical treatment.5
Mycotic aneurysms account for 2% of all coronary aneurysms. In most cases, they are a complication of bacterial endocarditis affecting the aortic and/or mitral valve. The most frequently isolated microorganisms are Staphylococcus aureus and Streptococcus viridans. Small aneurysms may respond favourably to early antibiotic treatment, but surgery is normally necessary to repair them.
To date, the publications we reviewed contain no reported cases of mycotic coronary aneurysms caused by S pneumoniae. In our case, we cannot confirm that this is a case of a superinfected aneurysm since the histological study of the cultured sample was negative (after antibiotic treatment), but its rapid growth and the association with purulent pericarditis make infection the most probable diagnosis.