Mortality from myocardial infarction is declining in high income countries, but the magnitude of this decline could differ between countries. We sought to compare the mortality trends from myocardial infarction between Spain and the United States.
MethodsThis was an observational retrospective study. Crude data were obtained from public databases. Standardized mortality rates were calculated for the last 17 years available for both countries (1990 to 2006), and stratified by age and sex. Joinpoint regression analysis was used for the trends analysis and projections.
ResultsThere has been a steady decline in mortality from myocardial infarction in both countries from 1990 to 2006. However, the magnitude of this decline was greater in the United States (relative reductions in men: 42.7% [Spain] and 59.7% [United States], and in women: 40% [Spain] and 57.4% [United States]). The estimated annual percentages of decline in mortality were greater in the United States (men: −10.7%, women: −5.1%) than in Spain (men: −1.9%, women: −5.1%). Projections for 2012 suggest that the mortality from myocardial infarction will be lower in men in the United States (53.33/100 000) than in Spain (81.52/100 000), while for women it will be equal (32.56/100 000 in the United States and 33.56/100 000 in Spain).
ConclusionsThe decline in mortality from myocardial infarction has been more pronounced in the United States than in Spain, and projections for upcoming years suggest in the United States it will evolve to rates below those expected in Spain for men and equal rates for women.
Keywords
Cardiovascular disease (CVD) is the leading cause of mortality in high income countries, and is showing a continuous increase in low and middle income countries as well. However, trends towards a decline in mortality from CVD have been described over recent decades.1, 2, 3 A recent analysis of the Framingham population has confirmed a decline in cardiovascular mortality in men and in women with or without diabetes mellitus.4
Mediterranean countries such as Spain have been historically considered as of “low risk” for CVD, showing lower cardiovascular mortality rates than other Western European countries or the United States (US),5 and specific risk charts are applied when estimating cardiovascular risk in individuals from these countries.6, 7 Mortality due to ischemic heart disease has been systematically higher than that due to cerebrovascular disease both in the US and in European countries, and although cardiovascular mortality rates also are declining in Mediterranean countries this reduction could be less pronounced than that seen in the US.5
In this study, we describe the trends in mortality from myocardial infarction (MI) in the US and in Spain and project the estimated mortality rates for upcoming years.
MethodsThis is a trend analysis. The main objective was to describe the trends in mortality from MI in a Mediterranean country (Spain) and in the US. Crude data for Spain and the US were obtained from the National Statistics Institute (Instituto Nacional de Estadística) and Center for Disease Control and Prevention, respectively. The analyzed codes for acute MI were 055 Infarto agudo de miocardio for the Spanish INE and International Classification of Diseases 10, I21 and I22 for the US Center for Disease Control and Prevention data. The analysis comprised the last 17 years available for both countries (1990 to 2006), and data were stratified by age and sex.
The crude mortality rates from MI for each year were calculated by dividing the total number of deaths due to MI by the actual population that year. The standardized mortality rate is the measure used to assess the relative mortality of a disease in comparison with the general population. Country rates were compared by obtaining the standardized mortality rates based on the world standard population. This way, the estimated number of deaths was calculated using the country mortality rates and the reference population. Indirect standardization was performed using age- and sex-specific population rates with the confidence intervals for the standardized mortality rate, allowing an estimation of the mortality from MI in Spain under the assumption of an age and sex population distribution similar to that of the US.
For the trends analysis and projections, joinpoint regression analysis was applied using the software provided by the Surveillance Research Program of the US National Cancer Institute.8 This regression model allows identification of points where a significant change in the linear slope of the trend occurred. In the model, each joinpoint informs of a significant change in the slope. The estimated annual percent change is then computed for each of those trends by fitting a regression line to the natural logarithm of the rates, using calendar year as a variable.
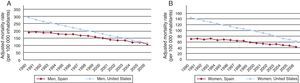
ResultsThe adjusted mortality rates for MI in Spain and the US are displayed in Table 1 and Figure 1. In Spain, the age-standardized mortality from MI in men decreased from 190.68 deaths/100 000 in 1990 to 109.21/100 000 in 2006 (a relative reduction of 42.7%). In the US, the figures for men were, respectively, 291.93 deaths/100 000 in 1990 and 117.54/100 000 in 2006 (relative reduction: 59.7%). Mortality due to MI in women from Spain decreased from 70.50 deaths/100 000 to 42.27/100 000 (relative reduction: 40%), whilst in the US it decreased from 144.05 deaths/100 000 to 61.37/100 000 (relative reduction: 57.4%).
Table 1. Age Adjusted Mortality Rates From Myocardial Infarction in Spain and United States (Deaths/100 000 Inhabitants)
| Year | Men | Women | ||||
| Spain | United States | 95%CI Spain vs US | Spain | United States | 95%CI Spain vs US | |
| 1990 | 190.68 | 291.93 | 187.47-193.89 vs 290.26-293.60 | 70.50 | 144.05 | 68.91-72.09 vs 143.09-145.01 |
| 1991 | 192.79 | 277.17 | 189.60-195.98 vs 275.56-278.78 | 71.26 | 139.24 | 69.68-72.84 vs 138.31-140.18 |
| 1992 | 187.95 | 264.20 | 184.82-191.07 vs 262.65-265.76 | 68.74 | 132.29 | 67.22-70.27 vs 131.38-133.19 |
| 1993 | 188.65 | 255.50 | 185.56-191.75 vs 253.98-257.01 | 71.38 | 127.96 | 69.84-72.92 vs 127.08-128.85 |
| 1994 | 178.33 | 243.70 | 175.35-181.31 vs 242.23-245.16 | 66.99 | 123.72 | 65.52-68.46 vs 122.86-124.58 |
| 1995 | 176.41 | 233.19 | 173.47-179.34 vs 231.77-234.61 | 68.61 | 118.64 | 67.14-70.08 vs 117.80-119.47 |
| 1996 | 176.82 | 221.89 | 173.90-179.73 vs 220.52-223.26 | 66.24 | 114.73 | 64.80-67.67 vs 113.91-115.55 |
| 1997 | 167.49 | 210.12 | 164.68-170.30 vs 208.79-211.44 | 64.36 | 108.01 | 62.96-65.76 vs 107.22-108.80 |
| 1998 | 165.56 | 200.34 | 162.79-168.34 vs 199.06-201.61 | 63.76 | 104.44 | 62.40-65.13 vs 103.68-105.21 |
| 1999 | 157.84 | 190.42 | 155.18-160.49 vs 189.20-191.65 | 58.51 | 100.83 | 57.22-59.81 vs 100.09-101.58 |
| 2000 | 149.648 | 180.32 | 147.07-152.22 vs 179.13-181.50 | 56.11 | 96.71 | 54.85-57.36 vs 95.99-97.44 |
| 2001 | 139.45 | 166.88 | 136.99-141.90 vs 165.76-168.01 | 53.61 | 90.28 | 52.39-54.82 vs 89.58-90.97 |
| 2002 | 136.11 | 159.18 | 133.71-138.50 vs 158.10-160.26 | 52.05 | 85.60 | 50.87-53.22 vs 84.93-86.27 |
| 2003 | 134.64 | 148.22 | 132.29-136.99 vs 147.18-149.25 | 52.22 | 79.23 | 51.05-53.39 vs 78.59-79.87 |
| 2004 | 122.40 | 134.47 | 120.17-124.62 vs 133.50-135.45 | 48.48 | 71.61 | 47.37-49.59 vs 71.01-72.21 |
| 2005 | 120.90 | 126.40 | 118.71-123.08 vs 125.46-127.33 | 46.77 | 67.43 | 45.68-47.85 vs 66.85-68.01 |
| 2006 | 109.21 | 117.54 | 107.15-111.27 vs 116.65-118.42 | 42.27 | 61.37 | 41.26-43.29 vs 60.82-61.92 |
95%CI, 95% confidence interval.

Figure 1. Observed adjusted mortality rates from myocardial infarction in the United States and Spain (period: 1990 to 2006). A: Men. B: Women. Note that the axis scales are different.
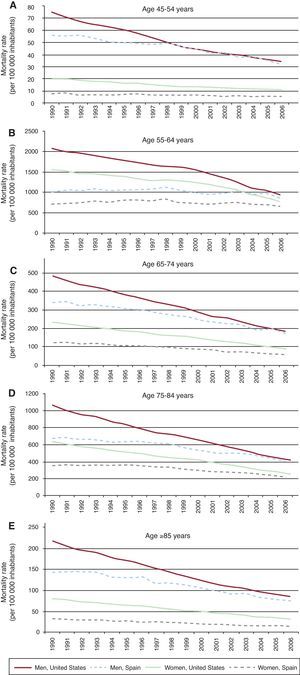
Figure 2 shows the adjusted mortality from MI stratified by ages. In the US population, a clear reduction in the mortality rates was observed for all ages in both men and women. The decline in mortality was more pronounced in the US than in Spain for all 5 age categories, especially in the elderly. Mortality rates in Spain were reduced for all the age categories except in those older than 85 years. The mortality rates in 1990 and 2006 and the relative reduction, stratified by age categories, are displayed in Table 2.

Figure 2. Observed mortality rates from myocardial infarction in the United States and Spain (period: 1990 to 2006) stratified by age categories. Note that the axis scales are different.
Table 2. Mortality Rates (Deaths/100 000 Inhabitants) and Relative Reduction From Myocardial Infarction in Spain and United States by Age Categories
| Spain | United States | |||||
| Years | Mortality rate 1990 | Mortality rate 2006 | Relative reduction, % | Mortality rate 1990 | Mortality rate 2006 | Relative reduction, % |
| Men | ||||||
| 45-54 | 55.55 | 32.27 | -41.90 | 74.49 | 34.20 | -54.09 |
| 55-64 | 141.96 | 74.67 | -47.40 | 216.44 | 85.60 | -60.45 |
| 65-74 | 339.26 | 169.22 | -50.12 | 483.51 | 181.90 | -62.38 |
| 75-84 | 674.67 | 408.23 | -39.49 | 1059.54 | 411.80 | -61.13 |
| ≥85 | 1005.26 | 857.23 | -14.73 | 2064.84 | 936.30 | -54.66 |
| Women | ||||||
| 45-54 | 7.45 | 5.13 | -31.12 | 19.88 | 11.20 | -43.65 |
| 55-64 | 31.95 | 13.98 | -56.23 | 79.86 | 32.60 | -59.18 |
| 65-74 | 121.56 | 55.24 | -54.56 | 231.87 | 88.10 | -62.01 |
| 75-84 | 355.08 | 217.14 | -38.85 | 634.68 | 255.60 | -59.73 |
| ≥85 | 710.23 | 657.82 | 7.38 | 1552.98 | 774.10 | -50.15 |
The findings from the joinpoint regression analysis over the period 1990–2006 for MI mortality are displayed in Table 3. The MI mortality rates declined more in both men and women (overall, an estimated annual percent decline of 5.5% per year and 10.7% per year for men in Spain and the US, respectively, and a decline of 1.9% per year and 5.1% per year for women in Spain and the US, respectively). The model shows a change in the slope in Spain in 1996 for men and in 1995 in women, whilst in the US the slope only drew a minor change for women in 2001 (Table 3).
Table 3. Joinpoint Analysis for Mortality From Myocardial Infarction in Men and Women
| Trend 1 | Trend 2 | |||
| Year | EAPC, % | Year | EAPC, % | |
| Men | ||||
| Spain | 1990-1996 | –2.97 | 1996-2006 | –6.43 |
| United States | 1990-2006 | –10.73 | — | — |
| Women | ||||
| Spain | 1990-1995 | –0.47 | 1995-2006 | –2.27 |
| United States | 1990-2001 | –4.73 | 2001-2006 | –5.92 |
EAPC, estimated annual percent of change.
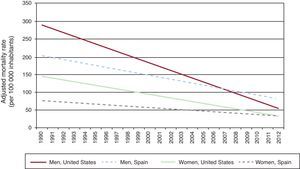
Table 4 and Figure 3 depict the age adjusted mortality from MI estimated for the period from 2007 to 2012. The estimated mortality from MI for men in the US will decrease below that estimated for men in Spain. In women, the mortality rates in the US will equal those of Spain. Estimated mortality rates from MI for men in 2012 of 81.52/100 000 in Spain and 53.33/100 000 in the US will yield expected relative reductions from 1990 of 57.2% in Spain and 81.7% in the US. For women, with an estimated mortality rate in 2012 of 33.56/100 000 in Spain and 32.56/100 000 in the US, the expected relative reductions from 1990 will be 52.4% in Spain and 77.4% in the US.
Table 4. Age Adjusted Estimated Mortality Rates (Deaths/100 000 Inhabitants) From Myocardial Infarction in Spain and United States From 2007 to 2012
| Men | Women | |||
| Year | Spain | United States | Spain | United States |
| 2007 | 108.86 | 106.98 | 43.06 | 58.03 |
| 2008 | 103.39 | 96.25 | 41.16 | 52.93 |
| 2009 | 97.92 | 85.52 | 39.26 | 47.84 |
| 2010 | 92.46 | 74.79 | 37.38 | 42.75 |
| 2011 | 86.99 | 64.06 | 35.46 | 37.65 |
| 2012 | 81.52 | 53.30 | 33.56 | 32.56 |

Figure 3. Observed (period: 1990 to 2006) and estimated (period: 2007 to 2012) mortality rate from myocardial infarction in the United States and Spain. The graphic is the result of joinpoint regression after simplification of the model by eliminating the observed changes in tendency. See text and Table 3 for complementary information.
DiscussionThis essentially descriptive study shows a steady decline in mortality from MI in both countries, Spain and the US, from 1990 to 2006. However, the magnitude of the decline in this period was greater in the US than in Spain (roughly 60% and 40% respectively), and the projections for 2012 suggest that the age-standardized mortality from MI in men will be lower in the US than in Spain, but rates will be equal for women.Over recent decades, trends towards a decline in mortality from CVD and in particular from MI have been described in the US, Canada, and western European countries.1, 2, 3, 4, 9 However, the magnitude of the reduction has so far been higher in the US. A recent study has analyzed the potential causes for such reduction in mortality,10 and concluded that approximately half of the decline may be attributable to reduction in major cardiovascular risk factors and half to proven efficacious medical therapies. This study described a decline in smoking prevalence, systolic blood pressure, total cholesterol, and physical inactivity but an increase in body mass index and diabetes mellitus, with a net effect of a decrease in the number of deaths from coronary heart disease.10 Changes in risk factors have been described as explaining factors for the mortality from MI trend in other industrialized countries.11, 12, 13, 14, 15
The recent evolution of the prevalence and control of major cardiovascular risk factors may explain, at least in part, the described trends in the US and Spain and why the decline in MI mortality is more pronounced in the US. High blood pressure has been described among the leading causes of global burden of disease in high income and in low and middle income regions16 and blood pressure levels are directly associated to coronary heart disease and cerebrovascular disease mortality.17 The burden of hypertension seems to have evolved more favorably in the US than in European countries. A study including the US, Canada, Spain, and 5 other European countries showed a lower prevalence of hypertension and a higher blood pressure control in the US than in European countries,18 with very different control figures in the US (blood pressure control over 60% of patients) than in Spain (scarcely over 20%). Recent studies in Spain have yielded better blood pressure control rates, but usually no higher than 40%,19 and underdiagnosis of hypertension is still significant in Spain.20 The different burden of blood pressure could, thus, be one of the factors accounting for the different trends in MI mortality in the US and Spain.
Dyslipidemia, and specifically high levels of low density lipoprotein cholesterol (LDL-C), increase cardiovascular morbidity and mortality; statin therapy achieves significant reductions in coronary heart disease incidence and mortality both in primary and secondary prevention.21, 22 In a recent study enrolling a total of 10 174 dyslipidemic adult patients on stable lipid-lowering therapy in 9 countries the proportion of patients attaining LDL-C target levels was 47.4% in Spain vs 75.7% in the US; the highest success rates were seen in Korea and the US and the lowest in France and Spain.23 In the NCEP Evaluation Project, 67% of 4885 patients achieved their LDL-C goal according to NCEP ATP III.24 Undertreatment with statins, given the proven benefit of these drugs, can be a barrier for a further reduction in cardiovascular events. Although reduction of cholesterol levels has been achieved in the US and in Spain, accounting for reductions in mortality in both countries, the higher reduction reached in the US and the larger employment of statins can explain in part the steeper US decrease in MI mortality.8, 25
Other cardiovascular risk factors may also account for the differences in the decline in MI mortality. Although the smoking habit is decreasing in industrialized countries, a recent World Health Organization report describes smoking habit in 37% and 27% of men and women in Spain, which contrasts with the figures for the US (25% men and 19% women).26 A number of factors can explain these differences. Health policies prohibiting smoking in indoor workplaces and public places have proven to be effective interventions for reducing smoking habit, but in Spain it wasn’t until 2006 that the first comprehensive smoke-free policy was implemented by the Spanish government27; other actions as smoking cessation programs are also less implemented in Spain. The problem becomes more complex involving cultural nuances, as in Spain smoking in men has declined while it has increased among women.28
The trend towards an increase in the prevalence of obesity and type 2 diabetes mellitus raises special concern. This worrisome trend has been described in both countries. In the US, the prevalence of diabetes has doubled from 1980 to 2004 in those aged more than 65 years, reaching a prevalence of more than 15% in this age group.29 A similar trend has been described in Spain, where the prevalence of type 2 diabetes has surpassed 20% in the elderly population.20, 30 This increase in the prevalence of type 2 diabetes is undoubtedly linked to the raising epidemic of obesity that is reaching Mediterranean countries too. In Spain, the prevalence of obesity in individuals aged 35-74 years was 29% in both men and women in a pooled analysis of 11 studies,30 and the prevalence of obesity and overweight in a population-based study in the elderly were 34.5% and 47.3%, respectively, leaving only a dismal 18.3% of individuals with normal weight.31 As the prevalence of obesity and type 2 diabetes is rising, consequences in terms of cardiovascular complications are expected to arise in coming decades. Along these lines, the recently reported increases in obesity prevalence both in adults and children by the World Health Organization is of particular concern in view of the impact that it may have in the future prevalence of cardiovascular and chronic diseases.32
The main limitation of our study is its descriptive nature, which precludes establishing a definitive relationship between the observed trends and the potential factors discussed in this section. However, the described factors and their modification have definitely proven to influence the incidence and mortality of coronary heart disease. Thus, one can speculate that the different epidemiology and control of major cardiovascular risk factors in both countries play a significant role in the different observed MI mortality trends.
We have focused our discussion on the differences in the epidemiology and control of major cardiovascular risk factors as the likely main cause for the different trends observed in the reduction of MI mortality. Other potential influential factors are more difficult to analyze. The acute care of patients with MI has improved in recent decades with reperfusion techniques being applied more frequently each year,10, 33 and socioeconomic barriers have been progressively eliminated in both countries.
The contribution of the aforementioned factors in the reduction of MI mortality in the US and in Spain have been analyzed by means of the IMPACT model.10, 25, 34 In the US, this modeling analysis showed the largest contribution to the mortality reduction to be explained by the decrease in major risk factors, and the reduction secondary to medical therapy due mostly to secondary prevention therapies.10, 33 More recently Flores-Mateo and coworkers have shown that the mortality reduction of coronary artery disease in Spain of almost 40% between 1985 and 2005 could be attributed to medical or surgical treatments in 47% and to risk factors prevention and control in 51% of cases. In total, the IMPACT model explained the mortality fall in 97% of cases. Secondary prevention was the most effective treatment in mortality reduction and cholesterol, blood pressure, and smoking reduction accounted for the major reduction related to risk factors.25 These studies agree in the importance of risk factors, both in terms of reduction in primary prevention and in terms of control in secondary prevention. The largest contribution to the decrease in MI deaths in both the US and in Spain was the reduction in cholesterol concentration8, 25 and this reduction was more steep in the US, as discussed above.
Although changes in mortality trends might be expected to happen in long-term intervals, new evidences have been recently published showing that declines in population mortality after individual intervention in cardiovascular risk factors can be achieved more quickly than traditionally has been perceived.35
One limitation of the study could be possible differences in the criteria used to codify the event (MI). Moreover, the causes of death can vary according to the physician that completes the mortality certificate. These are limitations always present in mortality studies, especially when comparing results between countries, that must be taken into account when interpreting results.
ConclusionsMortality from MI has decreased in the US and in Spain. However, although mortality from MI in the 90-s was higher in the US than in Spain, it has declined more steeply. The current situation shows a near-similar mortality from MI in Spain and in the US, and projections for upcoming years suggest that the age-standardized mortality from MI in men from the US will evolve to rates below those expected for men from Spain, while rates will be equaled for women. Epidemiological studies show different situations and trends in the prevalence and control of major cardiovascular risk factors in both countries that may account, at least in part, for the described trends. What we know about the epidemiology of cardiovascular risk factors and the findings described in this study should urge the administration and the medical community towards a more aggressive identification and correction of cardiovascular risk factors. On the other hand if obesity and diabetes prevalence continues growing, in the near future this observed decline in trends of mortality might change.
FundingThis paper was written at Loyola University of Chicago. The research was supported by a grant from the Valencian (Spanish) Ministry of Health.
Conflicts of interestNone declared.
Received 19 November 2011
Accepted 16 February 2012
Corresponding author: Departamento de Cardiología, Hospital Universitario San Juan de Alicante, Universidad Miguel Hernández, Ctra. Alicante-Valencia s/n, 03550 San Juan de Alicante, Alicante, Spain. vbertog@gmail.com