To the Editor:
Long QT syndrome (LQTS) arises from alterations of ion channels in the myocyte cell membrane and can be congenital or acquired. It is potentially serious because it can trigger a variety of ventricular tachycardia known as torsades de pointes. We present the case of a patient who followed a hypocaloric diet and developed a prolonged QT interval and torsades de pointes.
The 28-year old female patient had no relevant medical history, no family history of sudden death, and was slightly overweight. Two weeks earlier, she had started a very low-calorie weight loss plan for the first time, by which means she lost 4 kg in 10 days.
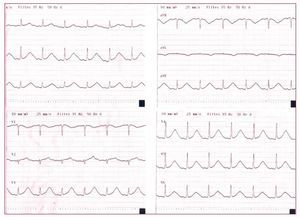
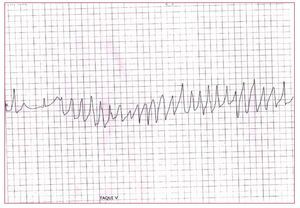
While resting, she experienced syncope and fell. She was conscious and aware of her surroundings in the emergency room, with a blood pressure of 100/60 mm Hg and a pulse rate of 76 beats/min; heart and lung auscultation was normal. The tests were normal, except for a potassium reading in the low end of the normal zone (3.4 mEq/L); magnesium and calcium levels were normal. The echocardiography did not show structural heart disease. The EKG on hospital admission (Figure 1) showed a corrected QT interval (QTc) of 740 ms. At 03:00 hours, she developed short bursts of torsades de pointes, which the patient perceived as rapid palpitations with dizziness (Figure 2). Treatment with magnesium sulphate and intravenous potassium supplements was given, and the arrhythmias progressively disappeared. The QTc interval remained long during 2 weeks, but no more arrhythmias developed. A previous EKG from the patient and from her close family members showed a normal QTc interval. Likewise, other causes of acquired LQTS were discarded, including the concomitant use of drugs, electrolytic changes and the existence of previous eating disorders. Two months after discharge from the hospital, the patient showed no symptoms and had a normal QTc interval.

Figure 1. Prolonged QTc interval (0.74 s) on admission to hospital.

Figure 2. Characteristic torsades de pointes.
LQTS arises because of alterations in the ion channels of the cardiac myocyte cell membrane, slowing ventricular repolarisation and prolonging the QT interval. This facilitates the appearance of early post-depolarization which can trigger torsades de pointes if a certain threshold is reached.
LQTS can be congenital, due to a gene mutation, or acquired, due to metabolic or electrolytic disorders (hypopotasemia, hypomagnesemia, hypocalcaemia), medication, intracranial hemorrhage, and more rarely eating and nutritional disorders, especially certain weight-loss diets.
In the case of individuals treated with weight-loss diets, prolonged QT interval, malignant ventricular arrhythmias, and sudden cardiac arrest have been described.1 The recorded cases are fundamentally those of women who had lost a significant amount of weight in a relatively short amount of time.2,3
Anorexia nervosa is a cause of sudden death among young women among whom a prolonged QT interval is found in up to 15% of the cases.4 Anorexic patients only present prolonged QTc when they have diselectrolytemia, generally hypopotasemia, or hypomagnesemia, but with a flat T-wave and associated with bradycardia.5,6 For our patient, the possibility of anorexia was discarded, which was added to an EKG typical of congenital LQTS, and not diselectrolytemia. Therefore, we cannot state whether it is a genetic defect worsened by the diet, or rather a totally acquired form. For this reason, it would be wise to carry out check-ups periodically and avoid drugs prohibited for congenital LQTS.
In our patient, it is probable that a genetic predisposition, not visible in the baseline EKG, added to being female and in combination with a strict hypocaloric diet, caused a prolongation of the QTc interval and the appearance of torsades de pointes.