To the Editor,
A 68-year-old man was admitted for dyspnoea at rest and ankle oedema. Chest x-ray showed bilateral pleural effusion. Electrocardiogram and routine laboratory tests were normal. Transthoracic echocardiography demonstrated an echogenic mass containing anechogenic areas involving the right atrium (RA) and right ventricle (RV), and causing a reduction of the right ventricle in-flow. Left ventricular (LV) dimensions and function were normal.
The patient was referred for cardiac magnetic resonance imaging (MRI).
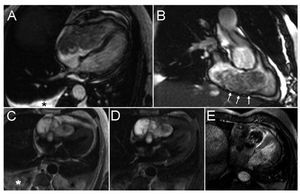
Dynamic imaging using steady-state free-precession cine MRI in the horizontal long-axis plane (Figure 1A) and in the right out-flow plane (Figure1B) showed a large (8 cmx13 cm) and inhomogeneous mass located in the RA and RV causing a reduction of RV inflow. Furthermore, there was akinesia of the basal and mid segments of the right anterior (Figure 1A) and right inferior ventricular walls due probably to the mass infiltration (Figure 1B).

Figure 1. MRI images with a variety of cardiac sequences. Steady-state free-precession cine MRI obtained along the horizontal long-axis (A) and in right ventricle outflow view (B). T1-weighted FSE images without (C) and with fat saturation (D). Contrast-enhanced inversion-recovery MRI obtained 10 minutes after contrast administration (E). Stars (*) indicate pleural effusion. White arrows on panel B show infiltration of the tumour in the RA and RV wall.
Tumour infiltration was observed, particularly in the RA and RV inferior wall (Figure 1B).
A T1-weighted fast spin-echo (Figure 1C) showed a multilobate strongly hyperintense mass. A T1 weighted image with fat saturation (Figure 1D) demonstrated that the hyperintensity was not due to fat and was an expression of the presence of metha-haemoglobin due to diffuse subacute-chronic haemorrhage.
Finally, delayed enhanced contrast inversion-recovery depicted an inhomogeneous enhancement involving almost exclusively the tumour periphery. On the other hand, a large part of the mass showed no significant delayed enhancement (Figure 1E). On the basis of the above findings, we made a presumptive diagnosis of a diffusely haemorrhagic malignant heart tumour suggestive of cardiac angiosarcoma.
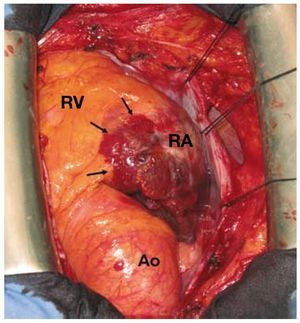
The patient was scheduled for surgery. However, at surgical exploration through median sternotomy, the mass appeared unsuitable for complete resection. The RA wall appeared completely invaded by the mass that was extending to the atrioventricular junction and to the anterior and posterior RV wall (Figure 2). Further surgical manoeuvres were withheld. Histology confirmed the diagnosis of primary cardiac angiosarcoma with intratumoural haemorrhage. The patient was then referred for medical treatment.

Figure 2. Intraoperative findings: Tumour infiltration of the right atrial wall. Infiltration of the atrioventricular groove and the right ventricle. Ao indicates aorta; RA, right atrium; RV, right ventricle.
Primary malignant cardiac tumours are rare. Sarcoma is the most common type (about 76%-78%) while angiosarcoma is the second most common type (about 31%).1,2 The symptoms are variable.3
Imaging morphology plays a key role in the preoperative differential diagnosis of cardiac tumours.4
The differential diagnosis is very broad and must include thrombus, vegetations, intracardiac metastases, infectious and nonbacterial thrombotic or marantic endocarditis as well as other sarcomas (unclassified spindle cell sarcomas, leiomyosarcoma, fibrosarcomas, malignant fibrous histiocytoma, mixoma). Discrimination between these pathologies by echocardiography may at times not give straightforward results. Use of a comprehensive MRI approach is helpful to characterize the different tissue components of angiosarcoma.
As in the reported case, some particular characteristics may help in recognizing an angiosarcoma on MRI:
1. Heterogeneous signal intensity originating from intra-tumoural hemorrhage
2. Heterogeneous enhancement and a cauliflower appearance on T1 weighted SE
3. A strong irregular enhancement appearance on contrast MRI