A 30-year-old male smoker of 20 cigarettes a day presented with a 1-hour history of chest tightness. ST elevation of 2mm was observed in the inferior leads of the electrocardiogram.
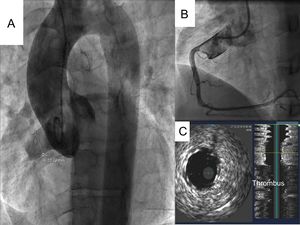
Emergency catheterization via the right radial artery was performed and a right Valsalva sinus aneurysm (VSA) was detected on angiography. The lesion was elongated and measured 13mm across, with extensive thrombotic material, but the right coronary artery (RCA), which was occluded at its origin, was not visualized (Figure 1).

After a guide catheter was inserted into the RCA, the proximal segment was predilated and a 4 x 28mm nondrug-eluting stent was implanted from the ostium (Figure 1B). Intravascular ultrasound showed correct stent apposition and a large amount of thrombotic material in the VSA (Figure 1C). It was decided to administer a fibrinolytic agent (tenecteplase) and perfuse tirofiban.
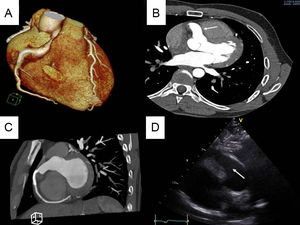
The patient's clinical outcome was satisfactory. At 24hours, chest computed tomography was performed, and the morphology of the aneurysm could be determined (27 x 14mm). No thrombotic remnants were apparent (Figure 2A and Figure 2B) and the RCA was patent (Figure 2C). The echocardiogram showed inferior hypokinesis and VSA free of thrombotic remnants (Figure 2D).

The patient was discharged after 5 days with warfarin and dual antiplatelet therapy. He was referred for surgical correction.
VSA is a rare cardiac defect that is usually congenital. The most frequent complication is rupture, but rare cases of thrombosis have also been reported, as in our case, leading to coronary ischemia and requiring emergency intervention.