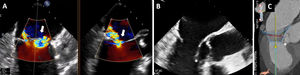
A 76-year-old man with symptomatic severe degenerative mitral regurgitation, and left ventricular ejection fraction of 50% (figure 1A), was put forward for percutaneous valve replacement (Tendyne, Abbott Vascular, USA) on the basis of his comorbidities and valve anatomy (multiscallop prolapse with very short posterior leaflet, after he provided informed consent). Computed tomography showed adequate annulus measurements and a neo-left ventricular outflow tract (LVOT) of 381mm2, but with an elongated anterior leaflet interfering with the virtual implant (figure 1B, C, arrow). Given the high probability of obstruction, it was decided to perform antegrade laceration of the anterior mitral leaflet (LAMPOON) immediately before prosthesis implantation.

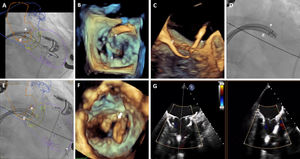
Via transeptal access, 2 deflectable sheaths were advanced to the left atrium. Through one of them, a snare was positioned in the LVOT and, through the other, a guide catheter was passed and an Astato XS20 guidewire (Asahi Intecc, Japan) was advanced until it was over the base of the A2 scallop. The electrified guidewire was advanced to cross the anterior leaflet (*), captured with the snare in the LVOT (#), and a rail was created around the anterior mitral leaflet (figure 2A-E). Using traction from both catheters and electrifying the previously-created rail, the leaflet was lacerated (figure 2F, videos 1 and 2 of the supplementary data). Finally, the Tendyne-LP-35M prosthesis was deployed as per usual technique, with no obstruction of the neo-LVOT (figure 2G, video 3 of the supplementary data).

To our knowledge, this is the first case in this country of a Tendyne implant facilitated with antegrade LAMPOON, an additional technique that can reduce anatomical exclusions for percutaneous transcatheter valve replacement.
AUTHORS’ CONTRIBUTIONSR. Estévez-Loureiro, R. Alarcón, and M. Barreiro-Pérez wrote the article, and all the authors approved the final version of the article.
FUNDINGNone.
CONFLICTS OF INTERESTNone.