The coronavirus disease 2019 (COVID-19) pandemic has changed how we view our consultations. To reduce the risk of spread in the most vulnerable patients (those with heart disease) and health personnel, most face-to-face consultations have been replaced by telemedicine consultations. Although this change has been rapidly introduced, it will most likely become a permanent feature of clinical practice. Nevertheless, there remain serious doubts about organizational and legal issues, as well as the possibilities for improvement etc. In this consensus document of the Spanish Society of Cardiology, we attempt to provide some keys to improve the quality of care in this new way of working, reviewing the most frequent heart diseases attended in the cardiology outpatient clinic and proposing some minimal conditions for this health care process. These heart diseases are ischemic heart disease, heart failure, and arrhythmias. In these 3 scenarios, we attempt to clarify the basic issues that must be checked during the telephone interview, describe the patients who should attend in person, and identify the criteria to refer patients for follow-up in primary care. This document also describes some improvements that can be introduced in telemedicine consultations to improve patient care.
Keywords
A new coronavirus with high infection and mortality rates, detected for the first time in December 2019 in Wuhan (China), is the cause of the SARS-CoV-2 (COVID-19) pandemic of 2020. The epidemiological situation and the steady increase in infections led to the declaration of a state of alarm and health care emergency in Spain on March 14, 2020.
The COVID-19 pandemic is causing considerable upheaval in our lives, particularly in health care and more specifically in cardiology. Indeed, the change already induced in outpatient cardiology care will continue in the near future, and telemedicine consultations have already acquired a new prominence. Accordingly, this consensus document has been created by the following groups to provide guidance for cardiologists facing the challenges generated by this new approach to outpatient heart disease care: the Clinical Cardiology Association, the Ischemic Heart Disease and Acute Cardiac Care Association, the Heart Failure Association, and the Heart Rhythm Association of the Spanish Society of Cardiology. Other contributors included representative primary care physicians from the 3 scientific societies in Spain: Spanish Society of Family and Community Medicine (SemFYC), the Spanish Society of Primary Care Physicians (Semergen), and the Spanish Society of General and Family Physicians (SEMG) (appendix). For this task, we have examined various points of interest. The first aspect concerns the fundamental characteristics required by telemedicine consultations in cardiology to maximize efficiency. We then examine the principal distinctive features inherent to the coordinated follow-up of the most common diseases in cardiology consultations: ischemic heart disease, with particular emphasis on chronic coronary syndrome (CCS), heart failure (HF), and arrhythmias, especially atrial fibrillation (AF). Last, a section is dedicated to the future of consultations after the COVID-19 pandemic (“How can we change clinical outpatient follow-up for heart disease patients after the pandemic?”), given that many aspects of treatment will surely change.
HOW TO PROVIDE AN EFFICIENT AND CONCLUSIVE TELECONSULTATION?In the current epidemiological context, it has become necessary to suspend face-to-face elective outpatient care for cardiology patients. In this new situation, we are faced with a dilemma: on the one hand, we cannot expose high-risk heart disease patients to the infection but, on the other hand, we cannot delay care for those who have a higher chance of experiencing a cardiovascular event because of their clinical situation. To obtain outpatient care that is appropriate for the current context, we must be able to distinguish the 2 situations to protect some patients from infection while prioritizing the early treatment of others.1
The basic objectives of an efficient and decisive consultation are the following: prioritization of patients most needing care (identifying warning signs or destabilization of baseline values), identification of the most appropriate care approach for each patient (face-to-face or virtual), and fulfillment of a high percentage of the consultations already scheduled for this period, therefore preventing an accumulation of “lost” visits.
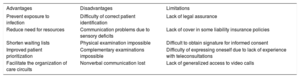
There are numerous advantages of teleconsultations.2 First, they avoid the exposure of both vulnerable patients and health care professionals to the infection. Second, they reduce resource use, shorten waiting lists, and prioritize patients most needing care, and are able to resolve problems,3 establishing a treatment plan and appropriate care circuit. Nevertheless, because the patients are not physically present, virtual consultations also have notable drawbacks, including difficulty in correct patient identification, communication problems due to possible sensory deficits, the impossibility of a physical examination or other tests, and the loss of nonverbal communication (table 1). To tackle these difficulties, we propose a teleconsultation that is as structured as possible and thus efficient and conclusive.
Advantages, disadvantages, and limitations of telemedicine consultations
| Advantages | Disadvantages | Limitations |
|---|---|---|
| Prevent exposure to infection | Difficulty of correct patient identification | Lack of legal assurance |
| Reduce need for resources | Communication problems due to sensory deficits | Lack of cover in some liability insurance policies |
| Shorten waiting lists | Physical examination impossible | Difficult to obtain signature for informed consent |
| Improved patient prioritization | Complementary examinations impossible | Difficulty of expressing oneself due to lack of experience with teleconsultations |
| Facilitate the organization of care circuits | Nonverbal communication lost | Lack of generalized access to video calls |
One important aspect of telemedicine is the role of nursing. We propose that nursing professionals make the first contact with patients, informing them that the scheduled consultation will be virtual (specifying the date and time), questioning them about any symptoms in order to inform the cardiologist of warning signs, evaluating if there are any sensory or communication deficits that would necessitate the presence of a family member at the consultation, asking patients to take their own biometric readings (blood pressure [BP], heart rate [HR], weight), and noting any medication they are presently taking, along with any questions that they may have for the cardiologist. The virtual consultation would be by telephone or video call, according to available resources.
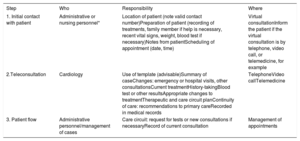
After this first contact, the cardiologist would perform the teleconsultation in the available format, preferably following a template that would structure the visit in the following sections: history-taking, evaluation of additional tests performed, summary of the case, and diagnostic and treatment decision-making. All of these steps must be correctly recorded in the medical records, as well as any additional tests requested or recommended to aid continuity of care. Each of these steps is outlined in table 2.
Practical proposals for teleconsultations
| Step | Who | Responsibility | Where |
|---|---|---|---|
| 1. Initial contact with patient | Administrative or nursing personnel* | Location of patient (note valid contact number)Preparation of patient (recording of treatments, family member if help is necessary, recent vital signs, weight, blood test if necessary)Notes from patientScheduling of appointment (date, time) | Virtual consultationInform the patient if the virtual consultation is by telephone, video call, or telemedicine, for example |
| 2.Teleconsultation | Cardiology | Use of template (advisable)Summary of caseChanges: emergency or hospital visits, other consultationsCurrent treatmentHistory-takingBlood test or other resultsAppropriate changes to treatmentTherapeutic and care circuit planContinuity of care: recommendations to primary careRecorded in medical records | TelephoneVideo callTelemedicine |
| 3. Patient flow | Administrative personnel/management of cases | Care circuit: request for tests or new consultations if necessaryRecord of current consultation | Management of appointments |
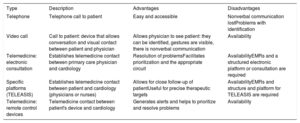
Different forms of teleconsultations are summarized in table 3, from less to more complex.
Different formats of telemedicine consultation in cardiology
| Type | Description | Advantages | Disadvantages |
|---|---|---|---|
| Telephone | Telephone call to patient | Easy and accessible | Nonverbal communication lostProblems with identification |
| Video call | Call to patient: device that allows conversation and visual contact between patient and physician | Allows physician to see patient: they can be identified, gestures are visible, there is nonverbal communication | Availability |
| Telemedicine: electronic consultation | Establishes telemedicine contact between primary care physician and cardiology | Resolution of problemsFacilitates prioritization and the appropriate circuit | AvailabilityEMRs and a structured electronic platform or consultation are required |
| Specific platforms (TELEASIS) | Establishes telemedicine contact between patient and cardiology (physicians or nurses) | Allows for close follow-up of patientUseful for precise therapeutic targets | AvailabilityEMRs and structure and platform for TELEASIS are required |
| Telemedicine: remote control devices | Telemedicine contact between patient's device and cardiology | Generates alerts and helps to prioritize and resolve problems | Availability |
EMR, electronic medical records; TELEASIS, home teleassistance platform.
This new form of virtual consultation offers a series of undoubted advantages, with distinguishing features for each type of heart disease. However, there are some aspects that must be resolved before a complete implementation of the approach, such as ethical and legal questions (legislative protection of virtual consultations beyond the health care emergency period) and professional aspects (loss of direct contact with patients). According to article 26 of the code of conduct,4 in the case of clinical examinations, teleconsultations are ethically acceptable if there is always a clear mutual identification of physicians and patients and in line with the confidentiality, safety, and secrecy norms outlined in the code. In fact, it must be highlighted that this type of care is not specifically regulated by any law and that not all civil liability policies include a specific clause concerning this practice.5 Thus, professionals should confirm their insurance coverage. However, we believe that this new form of consultation, once established, could become more normal in daily practice, which would oblige health care institutions to undertake a comprehensive regulation of the practice so as to dispel any doubts and to avoid possible legal loopholes.
TELEMEDICINE CONSULTATION IN PATIENTS WITH ISCHEMIC HEART DISEASEIschemic heart disease is one of the most common conditions in cardiology and one of the principal consultations.6 In addition, considerable evidence has linked ischemic heart disease to a worse COVID-19 prognosis.7 For this reason, we should prioritize any measures that minimize the risk of infection, mainly through the implementation of telemedicine visits.
Patient with acute coronary syndromeBefore patients with acute coronary syndrome (ACS) are discharged, they must be informed that their first consultation will be by telephone. In a detailed discharge report, the basic analytical tests should be scheduled (with time and date), with an electrocardiogram (ECG) to be performed in primary care, if necessary. At this point, patients should be shown how to take regular BP and HR readings. The quality of the discharge report is essential for an appropriate follow-up program to be coordinated with primary care.
Symptoms, treatment adherence, and possible adverse effects should be assessed in the first telephone consultation. Treatment optimization should be checked because it might not have been performed. In collaboration with cardiac rehabilitation, discharged patients should have been informed about the available programs, with priority given to telemedicine as a method of care, as proposed in the recommendations for cardiac rehabilitation in the de-escalation of the COVID-19 pandemic.8 During the consultation, an individual evaluation should consider the risk of unmonitored physical exercise, which will allow for low-risk patients to be selected for virtual coaching on physical exercise.
Follow-up consultations should include educational talks about disease, cardiovascular risk factors, diet, physical exercise, and sexual activity. These talks should be virtual and given by nursing staff (for both high- and low-risk patients). Due to their repetitive format, recorded material is advisable. These talks should dispel any doubts about treatments, and the use of video conferencing is advised, if available, ensuring that various patients can participate simultaneously. This not only optimizes time, but also allows for a particular patient's questions to help to clear up any doubts the others might not have thought of beforehand.
Online training regarding physical exercise should only be performed with low-risk patients. Video conferencing is also preferable and HR monitoring should be used to adjust the program to individual objectives.
In the case of possibly high-risk symptoms, patients should be selected for face-to-face consultations. They should be given the medical consultation alongside a nursing appointment for an ECG.
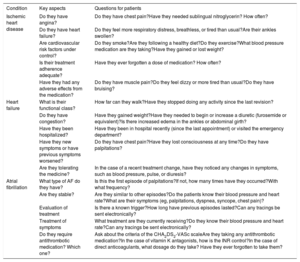
Patient with chronic coronary syndromeSeveral key aspects must be considered in the teleconsultation of CCS patients undergoing regular follow-up (table 4).
Basic questions that should be answered in a telephone interview with patients who have ischemic heart disease, heart failure, or atrial fibrillation
| Condition | Key aspects | Questions for patients |
|---|---|---|
| Ischemic heart disease | Do they have angina? | Do they have chest pain?Have they needed sublingual nitroglycerin? How often? |
| Do they have heart failure? | Do they feel more respiratory distress, breathless, or tired than usual?Are their ankles swollen? | |
| Are cardiovascular risk factors under control? | Do they smoke?Are they following a healthy diet?Do they exercise?What blood pressure medication are they taking?Have they gained or lost weight? | |
| Is their treatment adherence adequate? | Have they ever forgotten a dose of medication? How often? | |
| Have they had any adverse effects from the medication? | Do they have muscle pain?Do they feel dizzy or more tired than usual?Do they have bruising? | |
| Heart failure | What is their functional class? | How far can they walk?Have they stopped doing any activity since the last revision? |
| Do they have congestion? | Have they gained weight?Have they needed to begin or increase a diuretic (furosemide or equivalent)?Is there increased edema in the ankles or abdominal girth? | |
| Have they been hospitalized? | Have they been in hospital recently (since the last appointment) or visited the emergency department? | |
| Have they new symptoms or have previous symptoms worsened? | Do they have chest pain?Have they lost consciousness at any time?Do they have palpitations? | |
| Are they tolerating the medicine? | In the case of a recent treatment change, have they noticed any changes in symptoms, such as blood pressure, pulse, or diuresis? | |
| Atrial fibrillation | What type of AF do they have? | Is this the first episode of palpitations?If not, how many times have they occurred?With what frequency? |
| Are they stable? | Are they similar to other episodes?Do the patients know their blood pressure and heart rate?What are their symptoms (eg, palpitations, dyspnea, syncope, chest pain)? | |
| Evaluation of treatment | Is there a known trigger?How long have previous episodes lasted?Can any tracings be sent electronically? | |
| Treatment of symptoms | What treatment are they currently receiving?Do they know their blood pressure and heart rate?Can any tracings be sent electronically? | |
| Do they require antithrombotic medication? Which one? | Ask about the criteria of the CHA2DS2-VASc scaleAre they taking any antithrombotic medication?In the case of vitamin K antagonists, how is the INR control?In the case of direct anticoagulants, what dosage do they take? Have they ever forgotten to take them? |
AF, atrial fibrillation; INR, International Normalized Ratio.
Assessment of clinical stability is imperative. Symptoms should be assessed during the telephone interview. Chest pain and dyspnea are pivotal and patients suspected of having unstable angina or HF should be directed to an in-person consultation. They should be questioned about lifestyle-related factors, such as exercise, diet, and smoking. We should confirm that other cardiovascular risk factors are within target levels, such as BP (through self-measurement), low-density lipoprotein-cholesterol, or glycated hemoglobin; recent test results will need to be accessible in the electronic records. Treatment adherence should be evaluated, as well as potential adverse effects. Electronic prescription systems are helpful because they can show the level of adherence and pharmacological interactions and also allow for easy treatment modification.
If patients are receiving dual antiplatelet therapy, this regimen should be reviewed to determine if it should be ended at an earlier date or maintained beyond 12 months. If cardiovascular risk factor targets are not being met, lifestyle advice should be given and medication adjusted, if necessary. Intensification of antianginal therapy is reasonable if the patient has angina, particularly due to the recent results of the ISCHEMIA study,9 which found no prognostic benefit with invasive treatment in patients with CCS or moderate-to-severe myocardial ischemia. This study corroborates the predominant treatment approach in Europe for these patients, prioritizing the use of medication over intervention, which is highly relevant for teleconsultations during the COVID-19 pandemic.
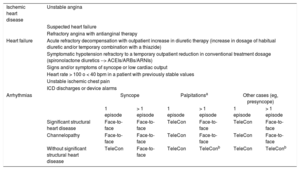
Patients who experience CCS decompensation or whose symptoms cannot be controlled should be directed to an in-person consultation (table 5).
Circumstances requiring a face-to-face consultation
| Ischemic heart disease | Unstable angina | ||||||
| Suspected heart failure | |||||||
| Refractory angina with antianginal therapy | |||||||
| Heart failure | Acute refractory decompensation with outpatient increase in diuretic therapy (increase in dosage of habitual diuretic and/or temporary combination with a thiazide) | ||||||
| Symptomatic hypotension refractory to a temporary outpatient reduction in conventional treatment dosage (spironolactone diuretics --> ACEIs/ARBs/ARNIs) | |||||||
| Signs and/or symptoms of syncope or low cardiac output | |||||||
| Heart rate > 100 o < 40 bpm in a patient with previously stable values | |||||||
| Unstable ischemic chest pain | |||||||
| ICD discharges or device alarms | |||||||
| Arrhythmias | Syncope | Palpitationsa | Other cases (eg, presyncope) | ||||
| 1 episode | > 1 episode | 1 episode | > 1 episode | 1 episode | > 1 episode | ||
| Significant structural heart disease | Face-to-face | Face-to-face | TeleCon | Face-to-face | TeleCon | Face-to-face | |
| Channelopathy | Face-to-face | Face-to-face | TeleCon | Face-to-face | TeleCon | Face-to-face | |
| Without significant structural heart disease | TeleCon | Face-to-face | TeleCon | TeleConb | TeleCon | TeleConb | |
ACEIs, angiotensin converting enzyme inhibitors; ARBs, angiotensin receptor blockers; ARNIs, angiotensin receptor neprilysin inhibitors; ICD, implantable cardioverter-defibrillator; TeleCon, teleconsultation.
If changes have been made to medication, BP and HR should be monitored, along with the development of any adverse effects; patients who have been appropriately trained should obtain their own measurements. One method of home monitoring that is becoming more and more widespread involves intelligent devices (mobile phone apps or smartwatches) that provide relevant information on different vital parameters.
Additional testing should be ordered only when strictly necessary. One limitation of these consultations concerns ECG availability. If necessary, the patient should be given an appointment in either the cardiology department or primary care. Reinforcement of monitoring at primary care level is important. In this context, online ECG systems must be highlighted because they allow for remote visualization from any location within the integrated health care system. It is necessary to once again highlight the importance of primary care access to integrated electronic medical records for coordinated and efficient follow-up.
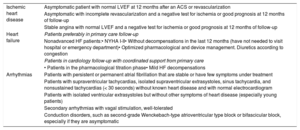
Stable patients should be directed to primary care for monitoring and follow-up, just as they would in face-to-face consultations. The criteria for cardiology discharge and follow-up in primary care are listed in table 6.
Cardiology discharge and primary care follow-up criteria for patients with ischemic heart disease, heart failure, or arrhythmias.
| Ischemic heart disease | Asymptomatic patient with normal LVEF at 12 months after an ACS or revascularization |
| Asymptomatic with incomplete revascularization and a negative test for ischemia or good prognosis at 12 months of follow-up | |
| Stable angina with normal LVEF and a negative test for ischemia or good prognosis at 12 months of follow-up | |
| Heart failure | Patients preferably in primary care follow-up |
| Nonadvanced HF patients:• NYHA I-II• Without decompensations in the last 12 months (have not needed to visit hospital or emergency department)• Optimized pharmacological and device management. Diuretics according to congestion | |
| Patients in cardiology follow-up with coordinated support from primary care | |
| • Patients in the pharmacological titration phase• Mild HF decompensations | |
| Arrhythmias | Patients with persistent or permanent atrial fibrillation that are stable or have few symptoms under treatment |
| Patients with supraventricular tachycardias, isolated supraventricular extrasystoles, sinus tachycardia, and nonsustained tachycardias (< 30 seconds) without known heart disease and with normal electrocardiogram | |
| Patients with isolated ventricular extrasystoles but without other symptoms of heart disease (especially young patients) | |
| Secondary arrhythmias with vagal stimulation, well-tolerated | |
| Conduction disorders, such as second-grade Wenckebach-type atrioventricular type block or bifascicular block, especially if they are asymptomatic |
ACS, acute coronary syndrome; HF, heart failure; LVEF, left ventricular ejection fraction; NYHA, New York Heart Association.
If a patient destabilizes during primary care follow-up, questions arise about complementary tests (eg, ECG, blood tests, echocardioscopy), or treatment adjustments are required, a consultation with cardiology should be performed to resolve any doubts. Regular cardiology consultations can then resume, preferably through telemedicine.
Patients with chronic coronary syndrome in primary care. Connection with cardiologyFor patients with ischemic heart disease and stable angina symptoms that have optimized treatment and have been already examined by cardiology, follow-up can be safely performed by the primary care physician.
Follow-up consultations should involve regular assessment of symptoms, cardiovascular risk, target achievement, and the possible development of comorbidities. An annual follow-up should be performed with blood testing, ECG, and, in some cases, an echocardiogram every 3 to 5 years (according to clinical features, ventricular function, valve disease, or other comorbidities).
Virtual nursing follow-up should be performed according to the level of intervention required and the self-care ability of the patients, with a predefined questionnaire including a series of questions. The values of BP and HR self-monitoring should be examined, as well as new treatments and any intercurrent processes from the previous appointment. Any necessary complementary tests should be requested.
There are 3 pathways through which patients would be directed to a follow-up teleconsultation with a primary care physician: a) patient is referred from a nursing consultation due to the onset of signs of destabilization; b) patient gets in contact by telephone because of a new symptom or decompensation; and c) patient requires treatment review or the results of complementary tests are available (blood test or ECG).
An electronic consultation should be performed with cardiology if there are doubts about the ECG or cardiac ultrasound (in both cases, the image files should be attached) or the blood tests, in the case of destabilization, and for treatment adjustments or requesting complementary tests not available in primary care (NT-proBNP, echocardiography, or others).
TELEMEDICINE CONSULTATION IN PATIENTS WITH HEART FAILUREPatients with HF are particularly vulnerable to infection from SARS-CoV-2, not only due to a higher risk of infection, but also because they have a worse prognosis if they are infected.7 This means that reorganization of care procedures to minimize in-person visits and prioritize telemedicine care is of the utmost importance to reduce the spread of the virus in these patients.10
Many face-to-face consultations for patients with HF can be replaced with teleconsultations. For this transformation to take place, resources that are already key to the follow-up of HF must be given even more prominence. Among these, the support of nursing personnel (hospital and primary care) in telemedicine is fundamental: they can instruct the patients about self-care and how to identify warning signs and to obtain basic biometric data at home, such as BP, HR, and weight, all of which help to provide more complete information for the teleconsultation.
One of the key questions is how to structure the telephone interview and what contents should be included for maximum efficiency. To simplify this task, and taking into account that one of the principal objectives is the identification of patients with signs and/or symptoms of decompensation, we propose 5 basic questions that should be answered (table 4).
It must be remembered that a SARS-CoV-2 infection can trigger acute HF decompensation.11,12 Thus, in addition to the abovementioned questions, it is important to be meticulous during the history-taking and to direct the questioning toward the presence of suspicious signs and symptoms, such as fever, dry cough, loss of taste or smell, upset stomach, and/or contact with suspected or confirmed COVID-19 cases.13
Teleconsultations usually allow for dose escalation during titration, but only when previous tolerance to the medicine has been demonstrated and there have been no adverse effects. A more gradual increase is also an option to avoid frequent blood testing; the priority is that the tests be conducted outside the hospital environment. Home extraction is preferable but, if not possible, the sampling should be performed in the local health center while both patients and health professionals strictly adhere to protective measures. Complementary testing should be postponed until considered necessary for decision-making (eg, echocardiogram for treatment optimization before device indication), although the approach should be individualized.
Teleconsultations also allow for the treatment of mild decompensation via medication dosage adjustment by telephone and with the support and coordination of primary care, but only when patients and their carers have been previously instructed about the medication used and trained to recognize symptom deterioration.
As is to be expected, not all patients can be treated with telemedicine alone: some will have to attend a face-to-face examination. Table 5 describes the clinical situations requiring an in-person consultation or a visit to the outpatient or emergency department.
In general, if a face-to-face visit is necessary, it should be done in a COVID-19-“free” area. If a day hospital is available, it is an excellent option as an alternative to hospitalization for patients seeking treatment for mild-to-moderate decompensation. They are usually “clean” areas that also permit parenteral administration of diuretics. Therefore, methods allowing for a more intense depletion should be chosen, such as hypertonic saline perfusion with furosemide, which safely achieves a greater volume of diuresis in less time,14 or elastomeric pumps, which allow for continual parenteral infusion for 5 to 7 days.15 These approaches mean that the patient is not obliged to return to the hospital on successive days.
Another pillar of outpatient care comprises primary care teams, especially in this era of a transformation toward a virtual and nonhospital care system. The coordination between levels of care is particularly important in guaranteeing the success of this new care format. Avoidance of hospital visits requires coordinated support from primary care not only in terms of the follow-up of stable chronic patients, but also in the coordination of care for mild decompensations and follow-up during titration, for example. Table 6 shows which patients would benefit from largely primary care follow-up and which ones would need shared follow-up between primary care and cardiology.
COORDINATED FOLLOW-UP OF OUTPATIENTS WITH ARRHYTHMIAAF is the most common arrhythmia in clinical practice. The clinical spectrum of AF is very broad and encompasses patients with hemodynamic instability and stable patients, whether in AF or sinus rhythm. Likewise, adequate prevention of thromboembolic complications is essential.16 The COVID-19 pandemic has obliged us to attempt to resolve most problems of AF patients through teleconsultations, even though we are conscious of their limitations. Any clinical telephone interview with patients should be well-structured and comprise the 5 basic questions proposed in table 4.
If patients are experiencing an AF episode (either first or recurrent), their hemodynamic stability should be evaluated, regardless of whether they are infected with SARS-CoV-2. If they are unstable, they will have to attend the hospital. In patients who are hemodynamically stable but infected with SARS-CoV-2, the strategy would be to monitor HR, with reassessment of the approach (eg, HR control vs cardiac rhythm control) once the infection has been overcome. In patients without infection, heart rhythm should be monitored and antiarrhythmic medication adjusted (dose escalation, extra dose) with later reevaluation. If the strategy comprises HR monitoring, negative chronotropic medication should be adjusted.16 In either of these cases, it would be very useful if the patient could inform the physician of their BP and HR values if possible, or even send electronic electrocardiographic data (from applications such as Kardia that record HR and heart rhythm).17
In any of the aforementioned cases, the key to patient prognosis is the prevention of stroke and systemic embolism; oral anticoagulation is indicated if the patient has a CHA2DS2-VASc score ≥ 1/2 (men/women).1 In the case of antithrombotic therapy, if the patient has good International Normalized Ratio (INR) control, a time in therapeutic range > 70%, and stable INR in the last 6 months, follow-up frequency can be reduced to diminish the risk of exposure to a possible SARS-CoV-2 infection. A switch to direct oral anticoagulants should be considered if the patient has inadequate INR control, has difficulties getting around, or is at high risk of infection, as are most patients with AF.1 If a patient with AF and anticoagulation criteria is discharged with a specific therapy for COVID-19 that interacts with the oral anticoagulation, low-molecular-weight heparin should be maintained at an anticoagulant dose. If the patient had previously been treated with vitamin K antagonists (with a good previous control and time in therapeutic range > 70%), they could resume the therapy, with low-molecular-weight heparin maintained at an anticoagulant dosage up to an INR ≥ 2 (2.5 in those with a metal prosthesis). In nonvalvular AF and prior poor INR control, difficulty in performing monitoring, or previous direct oral anticoagulant therapy, treatment with direct oral anticoagulants would be administered when the next dose of low-weight-molecular heparin is due.18 Following the recommendations of scientific societies during the COVID-19 pandemic, various health councils of Spanish autonomous communities have exceptionally allowed the initiation of direct oral anticoagulation in patients diagnosed with AF; this would reduce the frequent hospital visits that are necessary with vitamin K antagonist therapy.19
In the context of the current pandemic, telemedicine consultations are the preferred option for the diagnosis or follow-up of patients with other arrhythmias or their associated symptoms. In general, only patients with a short-term risk of destabilization should attend face-to-face consultations, distinguishing between:
- •
Patients diagnosed with arrhythmias. When the value of a face-to-face consultation is being assessed, the underlying heart disease, symptoms, and frequency should be taken into account (table 5).
- •
Patients in the diagnostic process for symptoms presumably produced by arrhythmias. Patients with frequent syncope episodes and/or any other compatible symptoms (eg, palpitations) that have required repeated emergency department care should be directed to in-person consultations.
Last, a hugely important facet involves determination of which patients should be treated on a priority basis by primary care physicians (table 6). This condition requires integrated clinical follow-up coordinated with primary care. Primary care is responsible for preventing the onset of AF by monitoring risk factors, obtaining an early diagnosis (and/or screening), the evaluation and initial treatment of symptoms through HR monitoring, prevention of stroke through anticoagulation (indication and follow-up), and assessment of drug tolerance and adherence during long-term follow-up.20 In general, the follow-up of patients with stable nonvalvular AF would be performed by the general practitioner and such patients would be referred to cardiology only if there was some complication requiring a more specialized approach.
WHAT WILL CARDIOLOGY CONSULTATIONS BE LIKE IN THE FUTURE?With the transition to a postpandemic phase, the key transformation in telemedicine will be the change from crisis mode (where untested or provisional technology is permitted) to a secure and sustainable approach that appropriately protects the information and privacy of patients and includes long-term technical support.21 According to a report from the consulting agency Oliver Wyman entitled, COVID-19: Telehealth is the “New Front Door”, > 65% of users are prepared to use telemedicine, although only 8% have done so before now.22
Health care practitioners are increasingly using tools such as WhatsApp to communicate with patients and/or other professionals about health care topics. Nevertheless, to avoid contravening data protection legislation, tools with data encryption must be used and only with the informed consent of the patient, recorded in the electronic medical records.23 Telemedicine generally provides appropriate levels of care and identifies which patients need treatment or additional support. According to some studies, up to 75% of face-to-face visits might be unnecessary or dispensable.24 For patients, a major advantage of telemedicine is continuity of care: after a face-to-face consultation, contact is often lost with the patient and their clinical condition is unknown until they attend the next care appointment. Telemedicine is finding its place in the field of cardiology as another tool for treating different cardiovascular diseases. As outlined above, achievement of therapeutic adherence and prevention of the recurrence of acute conditions are some of the possible improvements offered by telecardiology. This approach could also offer advantages in the care of cardio-oncological patients25 or those with diabetes mellitus.26
Telemedicine solutions implemented by cardiologists during the COVID-19 pandemicTelephone and video consultationsTelephone contact with patients before a face-to-face visit reinforces their essential self-management of their condition. Patients become more conscious of the basic aspects for monitoring their heart disease, such as BP, HR, body weight, and blood test results, including low-density lipoprotein-cholesterol, creatine, or glycated hemoglobin. Thus, it seems that the telephone consultation is here to stay.
Another option is to take another step forward and transform the telephone consultation into a video consultation. In some situations, visual contact aids communication and increases the flow of information. It permits examination of the presence of edemas in the lower extremities, respiratory effort, skin lesions, or medications. There are various ways to ensure the confidentiality and security required in clinical treatment through this method of contact. An example is a corporate user account with the Zoom Cloud Meeting application. These video consultations could be programmed, either by sending an invitation to the patient or carer, or directly through the application if the user already has the necessary device.
Email in cardiology consultationsAnother form of contact between patients and health practitioners is email. Test results, reports, and teleconsultation appointments could be sent through a secure account authorized by the institution. In addition, carers can send any doubts in writing for an approved solution, tables of vital signs or daily weight readings in HF consultations, or record any warnings that may come from the medical team.
Use of portable detectors (wearables)It was already relatively common for patients to have their own devices for reading BP or even oxygen levels. Nevertheless, the need for an electrocardiographic tracing to monitor the QTc interval in relation to the pharmacological therapy of COVID-19 has allowed portable devices such as the Kardia 6L27 to become a normal part of routine care in some settings. The device can quickly and easily provide a 30-second tracing of a bipolar ECG or a 6-lead limb ECG. The tracings can be sent to the physician by email. Various devices in development for the monitoring and clinical follow-up of cardiovascular diseases will certainly play key roles in cardiology.28
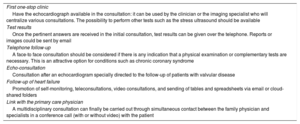
Reorganization of consultationsAlthough already a reality in many services, the need to reorganize the system to make it more efficient has become a new priority. Table 7 shows some proposals for incorporating technological communication advances into care practice in organizations.
Possible ways to reorganize cardiology consultations
| First one-stop clinic |
| Have the echocardiograph available in the consultation: it can be used by the clinician or the imaging specialist who will centralize various consultations. The possibility to perform other tests such as the stress ultrasound should be available |
| Test results |
| Once the pertinent answers are received in the initial consultation, test results can be given over the telephone. Reports or images could be sent by email |
| Telephone follow-up |
| A face-to face consultation should be considered if there is any indication that a physical examination or complementary tests are necessary. This is an attractive option for conditions such as chronic coronary syndrome |
| Echo-consultation |
| Consultation after an echocardiogram specially directed to the follow-up of patients with valvular disease |
| Follow-up of heart failure |
| Promotion of self-monitoring, teleconsultations, video consultations, and sending of tables and spreadsheets via email or cloud-shared folders |
| Link with the primary care physician |
| A multidisciplinary consultation can finally be carried out through simultaneous contact between the family physician and specialists in a conference call (with or without video) with the patient |
The COVID-19 pandemic has obliged health care systems to quickly implement telemedicine services that minimize the risks of infection for both patients and health care personnel, but some of these changes will probably remain, with patient care changed for good.
This health care crisis is clearly altering the classic concepts of medical care, and new technologies are emerging very quickly. However, it is vital to remember the necessary phases of the transformation and the best way to implement telemedicine safely and effectively. Once these technologies have been implemented, a regular evaluation of results is key to knowing where we are and where we want to go.
Finally, it is essential to stress that the adaptation to the new situation must be managed appropriately and that the legislation pertaining to telemedicine consultations must be applied correctly and without any ambiguity to avoid any doubts or legal loopholes.
FUNDINGThis document was funded by an unconditional grant from Laboratorios Menarini, Pfizer and Novartis Farmacéutica, none of which intervened in any way or at any time in the development of this consensus document. The opinion and recommendations of the experts are independent of the abovementioned funding.
CONFLICTS OF INTERESTThe authors declare no conflicts of interest in relation to this article.
Spanish Society of Cardiology (SEC): V. Barrios is coordinator of the Working Group on the Integration of Cardiology and Primary Care of the Cardiology Association. J. Cosín-Sales is President of the Clinical Cardiology Association. J.M. García-Pinilla is President of the Heart Failure Association. J. Jiménez-Candil is President of the Heart Rhythm Association. E. López-de-Sá is President of the Ischemic Heart Disease and Acute Cardiac Care Association. Á. Cequier is President of the Spanish Society of Cardiology.
Primary care societies: I. Egocheaga is Director of the Cardiovascular Section of the Spanish Society of General and Family Practitioners (SEMG) and V. Pallarés-Carratalá is Coordinator of the Working Group on Hypertension and Cardiovascular Disease of the Spanish Society of Primary Care Physician (Semergen).