Keywords
INTRODUCTION
This report presents the data for placement of implantable cardioverter-defibrillators (ICDs) reported to the Spanish Implantable Cardioverter-Defibrillator Registry in 2007. This registry was established in 1996 by the Electrophysiology and Arrhythmia Section (EAS) of the Spanish Society of Cardiology (SEC)1 prompted by the formation of the Working Group on ICD (WGICD) of the EAS of the SEC. This body was responsible for drafting this fourth official report with the cooperation of the majority of the hospitals in Spain that implant ICDs. Three official reports have been published previously. These cover activity during the 3-year period 2002-2004 and the years 2005 and 2006, respectively.2-4
METHODS
The registry data were obtained using a data collection form, which is available on the web page of the EAS of the SEC (www.arritmias.org). This form was completed directly and voluntarily by each implant team, during or after the implantation procedure, with the collaboration of the staff of the manufacturer of the ICD, and was sent to the SEC by fax or by e-mail. Data collection was primarily prospective. However, to make the registry more representative, in February 2008, a list of the implantations reported by each center in 2007 was sent to all the ICD implant centers that had contributed prospective data so that they could provide retrospective data on those patients for whom prospective data had not been made available to the registry.
Members of the SEC staff entered the data into the database of the Spanish ICD Registry. The data were cleaned by a SEC computer specialist and a member of the WGICD. Members of the current WGICD executive committee were responsible for data analysis and drafting this publication.
The population-based data used to calculate rates per million population, both on the national scale and according to autonomous community and province, were obtained from the estimations reported for the period up to January 1, 2007, by the National Institute of Statistics (http://www.ine.es).
To calculate to what extent the registry can be considered representative, we estimated the proportion of all the implants performed in Spain in 2007 that had been reported. To determine the total number of ICDs and replacements implanted in Spain, we used the data reported by the device manufacturers to the European Confederation of Medical Suppliers Associations (EUCOMED).
Where different medical conditions or clinical arrhythmias were reported for the same patient, only the most serious condition was included for analysis.
For each variable analyzed, unless otherwise stated, percentages were calculated based on the total number of implants, when that information was available.
Statistical Analysis
The numerical results were expressed as means (SD). The relationships between quantitative variables were analyzed using a linear regression model. Qualitative variables were compared using the c2 test. A P value less than .05 was considered significant. The statistical analysis was carried out using the JMP statistical software program (version 5.0.1).
RESULTS
Response rates for the different fields of the data collection form ranged from 72.2% to 96.5% for the main variables included in the registry.
Participating Centers
A total of 88 centers that performed ICD implants contributed data to the registry (Table 1). Sixty-eight of them were public hospitals. Table 2 shows the number of public hospitals that returned data to the registry per million population in 2007 for each autonomous community.


Total Number of Implants
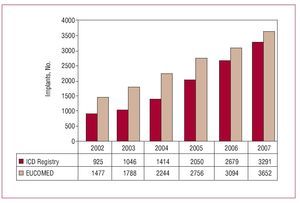
A total of 3291 implants (first-time, or primary implants, and replacements) were reported to the registry in 2007. Of these, 3180 (96.6%) were reported prospectively, whereas only 111 were reported retrospectively by 12 centers. Taking into account the fact that, according to EUCOMED data, a total of 3652 implants were carried out in that year, 90.1% of all implants performed in Spain were reported to the registry. Figure 1 shows the total number of implants reported to the registry and those estimated by the EUCOMED over the last 6 years.

Figure 1. Total number of implants reported to the registry and estimated by the European Confederation of Medical Suppliers Associations (EUCOMED) from 2002 to 2007. ICD indicates implantable cardioverter defibrillator.
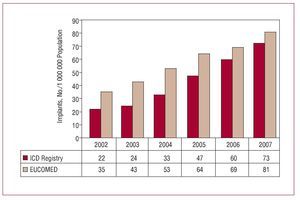
A total of 72.8 implants were reported to the registry per million population, whereas the number of ICD implanted per million population according to EUCOMED data was 80.8. Figure 2 shows the increase in the number of implants per million population reported to the registry and that estimated by the EUCOMED in the last 6 years. The number of implants reported to the registry by each implant center appears in Table 1. Table 3 shows the number of implants performed according to autonomous community, as reported to the registry in 2007, and the number of reported implants per million population. The number of implants reported to the registry and the number per million population, according to the provinces and autonomous communities in which the patients resided, are shown in Table 4.

Figure 2. Total number of implants per million population reported to the registry and estimated by the European Confederation of Medical Suppliers Associations (EUCOMED) from 2002 to 2007. ICD indicates implantable cardioverter defibrillator.



The majority of the reported implants (3036, or 95.3% of the total of 3187 reported to the registry in which the name of the hospital was provided) were carried out in public hospitals.
There was a correlation, which was almost statistically significant, between the number of hospitals where implantations were done per million population and the number of ICDs implanted per million population in each autonomous community (r2=0.63; P=.06). There was a weak correlation between the number of hospitals where implants were done per million population (r=0.3; P=.009).
Primary Implants Versus Replacements
Information on whether the procedure was a primary one was available for 3070 forms received (93.3%). Primary implants accounted for 2368 procedures, that is, 77.1% of the all recorded implantations. The number of primary implants reported to the registry per million population was 52. The number of replacement procedures was 702 (22.9%).
Age and Sex
The mean age of the patients, including those who received a primary implant and those who received a replacement ICD, was 61.2 (12) years (range, 3-92 years). These findings were very similar in the case of primary implants: 60.8 (13) years (range, 3-90 years). The majority of the patients were men (83.7% of the total and 83% in the case of primary implants).
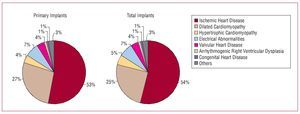
Underlying Heart Disease, Left Ventricular Ejection Fraction, Functional Class, and Baseline RhythmThe percentages of the different heart diseases were very similar in both the patients who underwent primary implantation and in the group as a whole (Figure 3). The most common condition was ischemic heart disease, followed by dilated cardiomyopathy, hypertrophic cardiomyopathy, and primary conduction abnormalities (Brugada syndrome, idiopathic ventricular fibrillation, and long QT syndrome). These were followed by valvular heart disease and arrhythmogenic right ventricular cardiomyopathy.

Figure 3. Underlying heart diseases reported to the registry (primary implants and total implants).
With regard to systolic ventricular function, almost half the patients had a left ventricular (LV) ejection fraction less than 30%. Somewhat more than one-quarter had a LV ejection fraction between 30% and 39%. The smallest group was that of patients with mild ventricular dysfunction, that is, with LV ejection fraction between 40% and 49% (Figure 4). There was a clear, almost significant, trend toward a higher proportion of patients with severe LV dysfunction (ejection fraction <30%) in the group that underwent primary implantation than in the group as a whole (49.1% vs 45.9%; P=.06 for comparison of the 4 groups of LV ejection fraction).

Figure 4. Left ventricular ejection fraction (LVEF) of the patients in the registry (primary implants and total implants).
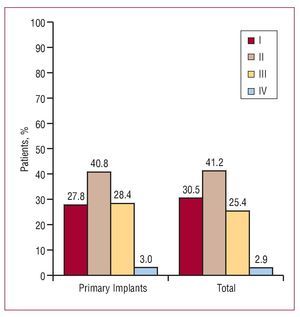
Somewhat over 40% of the patients were in New York Heart Association functional class II. They were followed in number by the group of patients in functional classes I and III, whereas only a very small number of patients were in functional class IV (Figure 5). In the group of primary implantations, there was an almost significant trend towards a greater proportion of patients in functional class III than in the overall group (28.4% vs 25.4%) due mainly to a smaller proportion of patients in functional class I (27.8% vs 30.5%; P=0.09 for the comparison of the 4 groups of functional class).

Figure 5. Functional class of the patients in the registry (primary implants and total implants).
The majority of the patients in the overall group (79%) were in sinus rhythm, whereas 15.6% had atrial fibrillation, 4.2% had pacemaker rhythm, and the rest exhibited other rhythms (atrial flutter or other atrial arrhythmias). These rates were similar in both the primary implant patients and the group as a whole (80.4%, 15.7%, and 3.5%, respectively).
Clinical Arrhythmia Requiring Implantation, Presentation, and Laboratory-Induced Arrhythmia
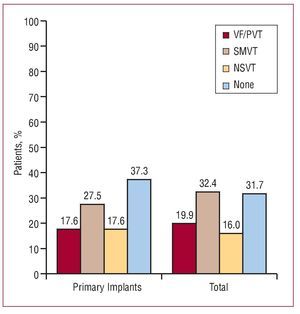
The absence of documented clinical arrhythmia was the most common finding among patients who underwent primary implantation. They were followed in number by those with sustained monomorphic ventricular tachycardia (SMVT). In the group as a whole, the proportion of both types was similar. The greater proportion of patients without documented clinical arrhythmia in the primary implant group versus the group as a whole (37.3% vs 31.7%) was statistically significant (P<.01; Figure 6). This was due mainly to the lower proportion of sustained arrhythmias in the group as a whole.

Figure 6. Clinical arrhythmia of the patients in the registry (primary implants and total implants). NSVT indicates nonsustained ventricular tachycardia; SMVT, sustained monomorphic ventricular tachycardia; VF/PVT, ventricular fibrillation/paroxysmal ventricular tachycardia.
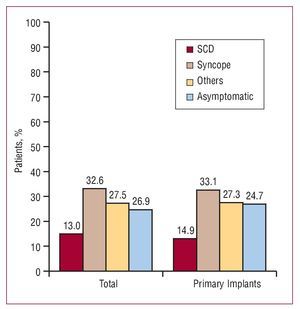
The most common clinical presentation, both in the group as a whole and among patients who underwent primary implantation, was syncope, followed by "other symptoms" and the absence of symptomatic arrhythmias. Although there was a tendency towards a greater proportion of asymptomatic patients, from the point of view of arrhythmias, in the primary implant group, this difference was not statistically significant (26.9% vs 24.7%; P=.2) (Figure 7).

Figure 7. Clinical presentation of arrhythmia in the patients of the registry (primary implants and total implants). SCD indicates sudden cardiac death.
Information on whether an electrophysiological study was done was available for 74.2% of the patients receiving a primary implant. It was carried out in 532 (30.3%) of the 1757 patients who underwent implantation for the first time and for whom this information was reported. In most cases, it was performed in the context of secondary prevention in patients who had had a previous infarction or those with dilated cardiomyopathy and SMVT; SMVT was the arrhythmia most frequently induced (54%). No sustained arrhythmia was induced in 32% of the studies.
Indications
The most common indication for ICD placement was ischemic heart disease and previous infarction. In this group, the indication for secondary prevention is slightly greater than for primary prevention, although primary prevention was the indication in 41.8% of the cases in which this information was available. The next most common indication in descending order of frequency was primary prevention in patients with dilated cardiomyopathy, who accounted for more than half the indications in this type of heart disease (55.2%). Among these cases, 58% of the implanted devices provided cardiac resynchronization therapy (CRT).
In patients with hypertrophic cardiomyopathy and Brugada syndrome, the majority of the indications were for primary prevention.
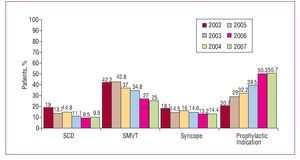
Table 5 details the changes in the incidences of the indications for the most prevalent heart diseases in the last 3 years (when the registry is most representative) and Figure 8 presents the changes in these indications, grouped together, over the last 6 years.


Figure 8. Changes in the major indications for implantable cardioverter defibrillators (primary implants) between 2002 and 2007. SD indicates aborted sudden death; SMVT, sustained monomorphic ventricular tachycardia; syncope, syncope without documented electrocardiographic evidence of arrhythmia.
Setting and Personnel
Information on setting and personnel was available for 94.2% of the primary implants and 93.1% of the replacements ones. Implantation was carried out in the catheterization laboratory in 63.7% of the cases and in the operating room in 36.3%. There were no reports of procedures done in other settings.
The implantations were carried out by electrophysiologists in 70% of the cases, by heart surgeons in 25.3% of the patients, and by other specialists in 4.7%.
Positioning of the Generator
In the majority of cases, the generator was implanted in a subcutaneous pectoral position (87.3% of all implants and 90.5% of the primary implants). The submuscular pectoral position was employed in 12% of the implants in the group as a whole and in 9.4% of the primary implants. Abdominal implantation was done in 3 primary implants and 18 replacements (0.1% of primary implants and 0.7% of all implants).
Device Type
When all the implants (primary implants and replacements) were analyzed, the percentages of single-chamber ICDs, dual-chamber ICDs, and CRT devices were 46.6%, 24.1%, and 29.3%, respectively. When only primary implants were evaluated, these proportions were 46.5%, 23.4%, and 30.1%, respectively. According to the data provided by the EUCOMED, in 2007, 1760 single-chamber ICDs (48.2%), 784 dual-chamber ICDs (21.4%), and 1108 CRT devices (30.4%) were implanted.
Reasons for Replacement. Substitution of Electrodes in Replacement Generators, and Use of Additional Electrodes
Of the reported replacements, information on the reason for replacement was available in 76% of the cases. Of these, 85.7% were due to battery depletion and the remainder was due to complications. Of the replacements due to complications, 76% (n=79) took place within the first 6 months after implantation.
Information on the functioning of the original electrodes was available in 75% of the cases. The proportion of nonfunctioning electrodes was 10.4%. Half of the nonfunctioning electrodes were explanted.
ICD Programming
Antibradycardia pacing was primarily in VVI mode (46.7%), with VVIR mode being used in 11.8% of the cases, DDD in 23.7%, DDDR in 14.2%, and other pacing modes in 3.6% of the cases (mainly modes selected to reduce the percentage of ventricular pacing in dual-chamber devices).
The device was programmed for ventricular antitachycardia pacing in 86.2% of the cases, with a combination of ventricular and atrial pacing in 4.7%. Antitachycardia pacing was not programmed during implantation in 9.1% of the cases.
Both ventricular and atrial defibrillation or cardioversion therapies were programmed in 5.3% of the cases.
Complications
Seven deaths (1.5/1000 procedures), 2 cases of cardiac tamponade, and 3 cases of pneumothorax were reported during implantation. Other complications were reported in 12 patients (acute heart failure, high defibrillation thresholds, early electrode displacement, etc).
DISCUSSION
In 2007, the Spanish ICD registry has once again become more representative, exceeding 90% of the procedures performed for the first time. The data in the registry can therefore be considered a good reflection of the indications, clinical characteristics of the patients, implant parameters, type of device, programming, and complications of implanted ICDs in Spain, and a good reference for real clinical practice in these aspects. To an even greater extent than in previous years, almost all implantation procedures were reported prospectively. This achievement has been made possible through the efforts of professionals who have collaborated with the registry.
Comparison With Previous Years
With respect to previous years, the number of implant centers has remained stable. Nevertheless, the total number of implants reported to the registry and the number of implants per million population have continued to increase due to an increase in the number of implantations performed and the number reported to the registry. The proportion of primary implants has decreased slightly compared to 2007, and these procedures now account for 77.1% of all those reported compared to 80% the previous year. There have been no significant changes in the epidemiological characteristics of the patients, which are similar in terms of mean age and the marked predominance of the male sex. There has been a slight change however in terms of the heart disease presented by the patient with a relative reduction in the proportion of patients with ischemic heart disease and an increase in the number of those with dilated cardiomyopathy. Patients with severe or moderate-to-severe ventricular dysfunction continue to be in the majority along with those in functional class II and III, with the gradual increase of previous years being maintained, related to the increase in the number of prophylactic procedures.
With respect to the type of indications, in 2007, in contrast to previous years in which a progressive increase in prophylactic implants was seen, a leveling off occurred. The prophylactic indication, taking into account all heart disease, as in 2006, exceeded 50% of all implants, although the increase was modest (50.3% vs 50.7%).
This leveling-off was particularly evident in the group of patients with previous infarction, in whom such indications were fewer than the 42% of the previous year. Nevertheless, in patients with dilated cardiomyopathy, the growth in prophylactic indications in previous years has been maintained, although it was not as marked, and in 2007 this disease accounted for 55.2% indications in this group of patients. This growth has occurred mainly because of increased numbers of ICDs with CRT rather than conventional ICD devices. This finding contrasts with that reported in other European countries, where the number of prophylactic implants has continued to rise, probably because the clinical practice guidelines, which are based on the main primary prevention clinical trials, are more closely adhered to.5,6
The differences observed in the clinical characteristics between the primary implant group and the implant group as a whole reflects the greater proportion of implants for primary prevention in current clinical practice. The implant group as a whole included replacement ICDs implanted between 4 and 8 years earlier, a time when most of the indications for ICD placement in Spain were for secondary prevention. The greater current proportion of indications for primary prevention is explained by the almost statistically significant trend toward a greater percentage of patients with severe LV dysfunction in functional class III in the primary implant group, as well as a greater number of patients with no documented clinical arrhythmia and a tendency toward a greater proportion of asymptomatic patients in terms of arrhythmias in that group.
The number of ICDs plus CRT devices has continued to increase, as in 2006, particularly for primary prevention, which is the main indication for this type of device. The proportion of dual-chamber ICDs has also increased at the same time as the proportion of single-chamber ICDs has decreased.
The lack of differences in the percentage of ICDs with CRT in the implant group as a whole and primary implants can be explained mainly by the fact that many replacement ICDs involved switching a conventional ICD for an ICD with CRT.
There were no significant changes in terms of programming of antitachycardia pacing functions or the antibradycardia pacing mode, although it is once again of note the greater number of pacing modes for preventing ventricular pacing in patients without CRT.
Finally, the proportion of implants done in the catheterization laboratory by electrophysiologists has remained stable at approximately 70%. Likewise, the proportion of subcutaneous implantations has remained stable.
Comparison With Registries in Other Countries
The data provided by EUCOMED for 2007 (industry data on ICDs) includes implantation of ICDs and ICDs with CRT for Germany, Italy, the Netherlands, Denmark, Austria, Ireland, Belgium, Switzerland, France, Finland, Sweden, the United Kingdom, Norway, Portugal, and Spain. They indicate a mean number of implants per million population of 189, ranging from 89 implantation procedures in Spain (80.8 assuming the population according to the Spanish National Institute of Statistics on January 1, 2007 was 45.2 million and not 41 million as assumed by the EUCOMED) to 317 in Germany. The countries above the European average were Italy, with 273 implants per million population, the Netherlands (264), Denmark (199), and Austria (193). Below the European average were Ireland (170), Belgium (153), Switzerland (149), France (125), Finland and Sweden (both 109), the United Kingdom (104), Norway (101), and Portugal (91). The increase in the average number of implantation procedures compared to 2006 in all these countries was 15.6% for ICDs and 21.2% for ICDs with CRT, whereas in Spain, it was 13.3% and 30.7%, respectively. The mean proportion of ICDs with CRT as a percentage of all ICDs was 33%; in Spain it was 30%, and ranged from 43% in Italy and 19% in Finland.
Recently, the first results of the National Implantable Cardioverter Defibrillator Registry have been published in the United States. This registry was created in 2005 with the collaboration of the American College of Cardiology Foundation and the Heart Rhythm Society. Participation is mandatory for implantation procedures done for primary prevention (a requirement of the Center for Medicare and Medicaid Services) and voluntary for other indications.7 As with the Spanish registry, it collects demographic data of the patients and indications for ICD placement, and although it is only mandatory to return data for primary prevention, 73% of the centers (performing 88% of the implantations) submitted data for all types of indication. It was launched in 2006 and from April 2006 through July 2007 had collected data from 1318 hospitals in the United States and a total of 160 000 ICD procedures. In total, 79.2% of the implants reported were for prophylactic purposes, in marked contrast to the Spanish registry. The mean age of the patients was 68.3 (12.5) years, that is, older than the Spanish patients, and the percentage of men was slightly lower (74.1%). The most common heart disease was ischemia with prior infarction, accounting for 55.3% of the implants, followed by dilated cardiomyopathy (29.8%), percentages fairly similar to those in the Spanish registry. Forty-six percent of the patients were in functional class III and the mean ejection fraction was 27% (11%). The implantations involved devices with CRT in 37.5% of the cases and 38.8% were dual-chamber devices— higher figures than for Spain. Eighty-two percent of the implantation procedures were performed by electrophysiologists, also a greater proportion than in the Spanish registry. The American registry also gathers data on complications; mortality was similar to that reported for Spain (0.02%).
Data for 2007 for the other regular registries such as the Danish and Portuguese registries have not been published.8
Geographic Distribution and Regional Differences
The information in the 2007 ICD registry continues to indicate, as in the preceding year, that geographical differences exist in terms of the available resources, indications, and numbers of ICD implants in Spain. Seven autonomous communities exceeded the national average: Cantabria, Navarre, Castille-Leon, Madrid, Galicia, Valencia, and Aragon, the same as in 2006 except for one. Nevertheless, there is a slight trend towards an evening out of the differences compared to the data for 2006. In 2007, there was an almost significant trend toward a correlation between the number of implantation units per million population and the number of implants per million population in the different autonomous communities, and this correlation, although weaker, was significant at the provincial level. The number of implants per million inhabitants in most provinces with a hospital or hospitals with ICD implantation facilities was greater than in the provinces without such facilities. This observation is in line with that published by Fitch-Warner et al9 in a study of the variation between autonomous communities in terms of usage of cardiovascular technologies. This study drew attention to, among other things, the influence of the offer of health care in explaining the variation in the indications for cardiovascular technology, linked in turn to regional resources. It is likely that adherence to clinical practice guidelines, particularly with regard to prophylactic indications of ICDs and ICDs with CRT, would help explain part of this variation.
Limitations
The implants reported to the registry do not account for all those performed in Spain, but, given that they constitute more than 90% of the total, it can be considered representative of the nationwide situation. In addition, the regional differences should be interpreted with caution since the proportion of implantation procedures reported to the registry by some centers is low. Nevertheless, there are fortunately now few centers with marked differences between the procedures reported and those actually performed.
Information on most of the variables on the data collection form was provided in over 80% of the implants reported to the registry. However, in some centers this percentage was low, and so the validity might be lower. A positive aspect in this sense is that the percentage of completed fields of the collection form, which had decreased slightly in 2006, had improved in 2007.
The indications for ICD placement for primary prevention in patients with ischemic heart disease and dilated cardiomyopathy, as in previous years, have not been detailed according to indication (MADIT II, SCDHeF, etc), given that not all the information necessary for such a subdivision is available.
Finally, the complications reported only correspond to those occurring during the procedure itself, and those that may occur or be detected shortly afterwards, such as developing heart failure, hematomas, electrode displacements, and many pneumothorax, are not included.
CONCLUSIONS
The 2007 Spanish ICD Registry recorded 90% of the ICD implants performed in Spain, the highest percentage to date, and so the registry can be considered representative of the scale and indications for this procedure in our country. The number of implants reported to the registry has continued the growth of preceding years, reaching 72.8 per million population in 2007. This figure is still slightly below the mean for the most developed countries of the European Union, where the growth has been more marked over the last year. Implantation of ICD devices for primary prevention stabilized last year and still accounts for more than half the indications for the procedure. As in previous years, there are substantial variations in implantations within Spain.
ACKNOWLEDGMENTS
We would like to thank all of the health professionals involved in ICD implants in Spain who have voluntarily and disinterestedly submitted data on implants to the registry, the personnel of the different ICD manufacturers (Medtronic, Boston-Guidant, St Jude Medical, Biotronik, and Sorin Group) for their help in data collection and in sending the data collection forms for the majority of the implants to the SEC, and the SEC for its invaluable support in introducing data and in maintaining the registry, with special mention of Gonzalo Justes, José María Naranjo, and Miguel Ángel Salas.
ABBREVIATIONS
CRT: cardiac resynchronization therapy
EAS: Electrophysiology and Arrhythmia Section
EUCOMED: European Confederation of Medical Suppliers Associations
ICD: implantable cardioverter-defibrillator
SMVT: sustained monomorphic ventricular tachycardia
SEC: Spanish Society of Cardiology
WGICD: Working Group on Implantable Cardioverter-Defibrillators
Correspondence: Dr. R. Peinado Peinado.
Sección de Arritmias. Servicio de Cardiología. Hospital Universitario La Paz.
P.o de la Castellana, 261. 28046 Madrid. España.
E-mail: rpeinado@secardiologia.es