

The present article reports the characteristics and outcome of heart transplantation in Spain since it was first performed in May 1984.
MethodsWe provide a descriptive analysis of the characteristics of the recipients, the donors, the surgical procedure, and results of the heart transplantations performed in Spain until 31 December 2013.
ResultsDuring 2013, a total of 248 transplantation procedures were carried out, bringing the time series to a total of 7023 transplantations. The temporal analysis confirms a significant deterioration in the clinical profile of the recipients (higher percentage of older patients, severe renal failure, insulin-dependent diabetes mellitus, previous heart surgery, mechanical ventilation), of the donors (higher proportion of older donors and greater weight mismatch), and of the procedure (higher percentage of emergency transplantations which, in 2013, reached 49%, and with ischemia times > 240min). There was a marked increase in the use of circulatory assist devices prior to transplantation which, in 2013, were employed in 25.2% of all the patients. The survivals at 1, 5, 10, and 15 years were 76%, 65%, 52%, and 37%, respectively, and have remained stable since 1995.
ConclusionsHeart transplantation activity in Spain remains stable in recent years, with around 250 procedures a year. Despite the clear deterioration in the clinical characteristics of the donors and recipients, and lengthening of the operative times, the results in terms of mortality continue to be comparable to those reported in our neighboring countries, and a growing use of circulatory assist devices prior to transplantation is confirmed.
Keywords
Since 1991, the Spanish Heart Transplantation Registry (Registro Español de Trasplante Cardiaco [RETC]) has published a report on the clinical and surgical characteristics and the overall results of the heart transplantation procedures performed in Spain (Appendix).1–24 The present article describes the data corresponding to the population of patients undergoing transplantation up to 31 December 2013. The major strength of the RETC has been identified as the comprehensive inclusion and update of all the heart transplantation procedures performed in all the hospitals in Spain since May 1984, regardless of their characteristics and outcomes. Moreover, data are collected prospectively and stored in a common database, in accordance with criteria agreed on by consensus and updated by all the transplantation teams.
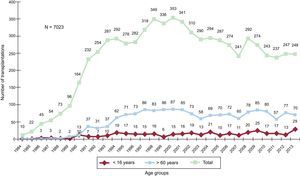
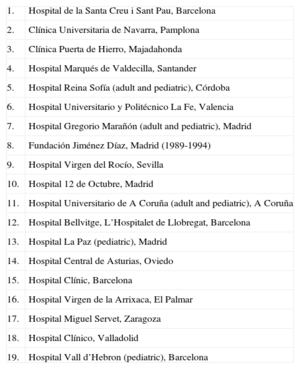
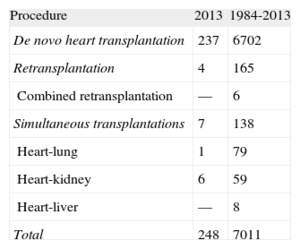
METHODSPatients and CentersOf the 19 centers that have contributed data to the RETC, 18 remain active at the present time (Table 1). The number of procedures performed each year is shown in Figure 1. The entire series encompasses 7023 procedures. Data, including follow-up information, are missing from the records of 12 cases, which have not been included in the analyses; thus, the final sample consisted of 7011 cases. Of the 248 procedures carried out, 29 (11.7%) were performed in pediatric patients (age<16 years). The types of procedures documented in 2013 and in the time series as a whole are summarized in Table 2.
Centers Participating in the Spanish Heart Transplantation Registry (1984-2013) (Listed in Chronological Order of the Performance of Their First Transplantation)
| 1. | Hospital de la Santa Creu i Sant Pau, Barcelona |
| 2. | Clínica Universitaria de Navarra, Pamplona |
| 3. | Clínica Puerta de Hierro, Majadahonda |
| 4. | Hospital Marqués de Valdecilla, Santander |
| 5. | Hospital Reina Sofía (adult and pediatric), Córdoba |
| 6. | Hospital Universitario y Politécnico La Fe, Valencia |
| 7. | Hospital Gregorio Marañón (adult and pediatric), Madrid |
| 8. | Fundación Jiménez Díaz, Madrid (1989-1994) |
| 9. | Hospital Virgen del Rocío, Sevilla |
| 10. | Hospital 12 de Octubre, Madrid |
| 11. | Hospital Universitario de A Coruña (adult and pediatric), A Coruña |
| 12. | Hospital Bellvitge, L’Hospitalet de Llobregat, Barcelona |
| 13. | Hospital La Paz (pediatric), Madrid |
| 14. | Hospital Central de Asturias, Oviedo |
| 15. | Hospital Clínic, Barcelona |
| 16. | Hospital Virgen de la Arrixaca, El Palmar |
| 17. | Hospital Miguel Servet, Zaragoza |
| 18. | Hospital Clínico, Valladolid |
| 19. | Hospital Vall d’Hebron (pediatric), Barcelona |
 and by age group.")
The database consists of 175 clinical variables, established by consensus among all the transplantation teams, which include data on the recipient, donor, surgical technique, immunosuppression, and follow-up. Since 2013, the data are introduced and updated electronically, in real time, by means of an application specifically designed for this purpose and available on the internet. The database support is a Microsoft Excel file. This procedure replaced the preceding approach, in which each center conveyed the data to the director of the registry by e-mail in Microsoft Access format. Database management, quality control, and statistical analysis are outsourced to a CRO (contract research organization), at the present time, ODDS, S.L.
Ethics committee approval, auditing, and registration with the Spanish Ministry of Health, Social Services and Equality meet the requirements of the Spanish Data Protection Law 15/1999.
Statistical AnalysisThe continuous variables are expressed as mean (standard deviation) and the categorical variables as percentages. The results were classified by transplantation year, an approach for which the overall sample was divided into six 5-year groups (1984-1988, 1989-1993, 1994-1998, 1999-2003, 2004-200, and 2009-2013). The between-group differences were analyzed using a nonparametric test for the time trend (Kendall's tau). Survival curves were calculated using the Kaplan-Meier test and were compared using the log rank test. A P value < .05 was considered to indicate a significant difference.
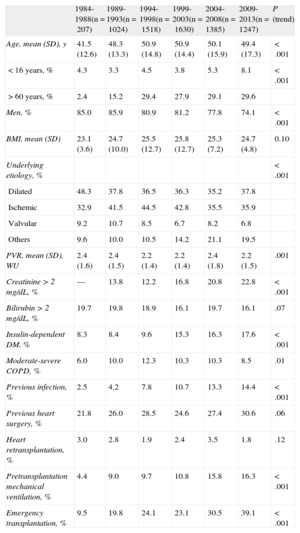
RESULTSRecipient CharacteristicsIn 2013, the recipients had a mean age of 47 (19) years (range, 0-70 years); 71% were men, and the most common underlying diagnoses were ischemic heart disease (33.6%), idiopathic dilated cardiomyopathy (37.2%), and valvular heart disease (8.1%), whereas the etiology of the remaining 21.1% varied. The characteristics of the patients corresponding to each transplantation period are summarized in Table 3. It is notable that 30% of the recipients in the most recent period were over 60 years of age and that more than 25% were women. There is also evidence of an increase in risk conditions such as renal dysfunction, diabetes mellitus, infection during the 15 days prior to transplantation, and the need for mechanical ventilation. In contrast, there was a significant trend toward a decrease in retransplantation in the most recent period, in which the rate was scarcely 2% of all the transplantation procedures, with an annual average of 2.4% for the entire time series.
Recipient Characteristics in the Spanish Heart Transplantation Registry (1984-2013)
| 1984-1988(n=207) | 1989-1993(n=1024) | 1994-1998(n=1518) | 1999-2003(n=1630) | 2004-2008(n=1385) | 2009-2013(n=1247) | P (trend) | |
| Age, mean (SD), y | 41.5 (12.6) | 48.3 (13.3) | 50.9 (14.8) | 50.9 (14.4) | 50.1 (15.9) | 49.4 (17.3) | <.001 |
| < 16 years, % | 4.3 | 3.3 | 4.5 | 3.8 | 5.3 | 8.1 | <.001 |
| > 60 years, % | 2.4 | 15.2 | 29.4 | 27.9 | 29.1 | 29.6 | |
| Men, % | 85.0 | 85.9 | 80.9 | 81.2 | 77.8 | 74.1 | <.001 |
| BMI, mean (SD) | 23.1 (3.6) | 24.7 (10.0) | 25.5 (12.7) | 25.8 (12.7) | 25.3 (7.2) | 24.7 (4.8) | 0.10 |
| Underlying etiology, % | <.001 | ||||||
| Dilated | 48.3 | 37.8 | 36.5 | 36.3 | 35.2 | 37.8 | |
| Ischemic | 32.9 | 41.5 | 44.5 | 42.8 | 35.5 | 35.9 | |
| Valvular | 9.2 | 10.7 | 8.5 | 6.7 | 8.2 | 6.8 | |
| Others | 9.6 | 10.0 | 10.5 | 14.2 | 21.1 | 19.5 | |
| PVR, mean (SD), WU | 2.4 (1.6) | 2.4 (1.5) | 2.2 (1.4) | 2.2 (1.4) | 2.4 (1.8) | 2.2 (1.5) | .001 |
| Creatinine > 2 mg/dL, % | — | 13.8 | 12.2 | 16.8 | 20.8 | 22.8 | <.001 |
| Bilirubin > 2 mg/dL, % | 19.7 | 19.8 | 18.9 | 16.1 | 19.7 | 16.1 | .07 |
| Insulin-dependent DM, % | 8.3 | 8.4 | 9.6 | 15.3 | 16.3 | 17.6 | <.001 |
| Moderate-severe COPD, % | 6.0 | 10.0 | 12.3 | 10.3 | 10.3 | 8.5 | .01 |
| Previous infection, % | 2.5 | 4.2 | 7.8 | 10.7 | 13.3 | 14.4 | <.001 |
| Previous heart surgery, % | 21.8 | 26.0 | 28.5 | 24.6 | 27.4 | 30.6 | .06 |
| Heart retransplantation, % | 3.0 | 2.8 | 1.9 | 2.4 | 3.5 | 1.8 | .12 |
| Pretransplantation mechanical ventilation, % | 4.4 | 9.0 | 9.7 | 10.8 | 15.8 | 16.3 | <.001 |
| Emergency transplantation, % | 9.5 | 19.8 | 24.1 | 23.1 | 30.5 | 39.1 | <.001 |
BMI, body mass index; COPD, chronic obstructive pulmonary disease; DM: diabetes mellitus; PVR, pulmonary vascular resistances; SD, standard deviation; WU, Wood units.
Unless otherwise indicated, data are expressed as mean (standard deviation).
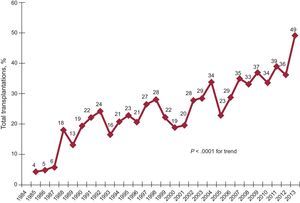
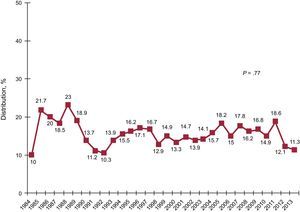
The percentage of emergency procedures has increased progressively and very significantly (P<.0001) over time (Figure 2), reaching 39% in the most recent period (Table 3). It is striking that, in 2013, nearly half of the procedures were performed in the emergency setting (Figure 2).
.")
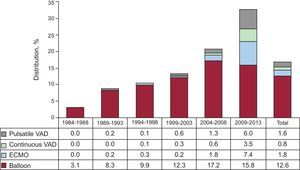
In 2013, an extracorporeal membrane oxygenator was used in 11.7% of the cases, continuous-flow ventricular assist devices in 6.0%, and pulsatile ventricular assist devices in 5.2%, Thus, in that year, the use of these devices (22.9%) nearly doubled that of balloon counterpulsation as the only method of assistance (13.3%) prior to transplantation. From 2004 on, there was a constant increase in the use of mechanical circulatory support other than the standard intra-aortic balloon counterpulsation. The distribution of the ventricular assist devices used in each period is shown in Figure 3.
Characterization of the Donors and Ischemia Time
In 2013, the mean age of the donors was 40.2 (16.1) years (44% were > 45 years of age) and 53.8% were men. In 25% of the cases, the donor body weight was 20% greater than that of the recipient, whereas the opposite was observed in 10.1%. In 27.8% of the cases, a male recipient received a graft from a female donor.
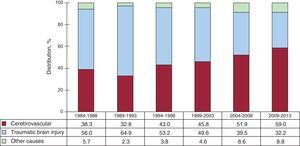
The donor characteristics corresponding to each 5-year period are shown in Table 4. The summary of the causes of donor death by period is provided in Figure 4. Over the course of the periods described, there was an increase in the report of stroke as the major cause of death, as opposed to traumatic brain injury.
Donor Characteristics and Ischemia Time in the Spanish Heart Transplantation Registry (1984-2013)
| 1984-1988(n = 207) | 1989-1993(n = 1023) | 1994-1998(n = 1517) | 1999-2003(n = 1630) | 2004-2008(n = 1385) | 2009-2013(n = 1247) | P (trend) | |
| Age, mean (SD), y | 24.7 (8.1) | 26.9 (10.5) | 30.2 (12.3) | 32.5 (13.0) | 34.6 (13.8) | 38.9 (14.6) | <.001 |
| Age > 45 years, % | 1.1 | 7.6 | 13.2 | 20.1 | 26.1 | 39.4 | <.001 |
| Men, % | 85.9 | 77.0 | 70.4 | 71.1 | 68.4 | 63.6 | < .001 |
| Female donor to male recipient | 11.7 | 18.8 | 22.3 | 19.7 | 20.6 | 21.4 | < .001 |
| Body weight, mean (SD), kg | 67.7 (12.0) | 69.6 (13.6) | 68.4 (16.0) | 71.3 (15.7) | 72.3 (18.0) | 71.6 (18.5) | < .001 |
| Recipient/donor weight, mean (SD) | 0.97 (0.19) | 0.98 (0.17) | 0.99 (0.22) | 0.98 (0.21) | 0.97 (0.21) | 0.94 (0.29) | .057 |
| Recipient/donor weight > 1.20, % | 10.5 | 11.1 | 16.0 | 12.3 | 12.2 | 8.2 | .02 |
| Recipient/donor weight < 0.8, % | 16.8 | 13.3 | 14.0 | 15.9 | 18.6 | 20.7 | .02 |
| Ischemia time, mean (SD), min | 132 (54) | 167 (61) | 182 (60) | 187 (63) | 202 (64) | 210 (62) | < .001 |
| < 120min, % | 48.5 | 22.6 | 18.6 | 17.3 | 12.9 | 9.4 | < .001 |
| 120-180min, % | 30.5 | 37.4 | 29.6 | 27.1 | 24.1 | 20.2 | |
| 180-240min, % | 18.0 | 30.2 | 37.6 | 35.9 | 36.8 | 41.5 | |
| > 240min, % | 3.0 | 9.8 | 14.2 | 19.7 | 26.2 | 29.0 |
SD, standard deviation.
Unless otherwise indicated, data are expressed as mean (standard deviation).

The ischemia time has become increasingly prolonged throughout the time series: in the most recent period (2009-2013), it was nearly 1.5h longer than in the initial period (1984-1988). From 2009 to 2013, the ischemia time in nearly 30% of the procedures was > 4h (Table 4). In 2013, the mean ischemia time was 209.1 (59.6) min, and the ischemia time was > 4h in 27.9% of the cases.
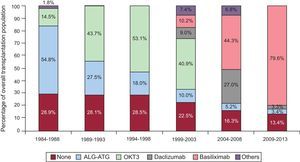
ImmunosuppressionIn 2013, 87.1% of the recipients received some type of induction immunosuppressive therapy, basiliximab in the great majority of cases (85.1%). Figure 5 shows that the administration of induction therapy has increased progressively to the extent that it is now used in the great majority of patients. In the period from 2009 to 2013, induction was achieved in 80% of the recipients with interleukin 2 receptor antagonists (basiliximab or daclizumab, mainly the former), which replaced OKT3 as the most widely used agent in earlier periods.

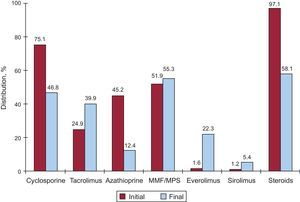
Initial immunosuppression in 2013 mostly consisted of tacrolimus (81.8%) as a calcineurin inhibitor, mycophenolate mofetil (97.1%) as an antiproliferative agent, and steroids (97.9%). Figure 6 summarizes the drugs used in initial immunosuppression and at the end of follow-up in the entire time series. After an average follow-up of 6.8 years, 58.1% of the patients continued to be treated with corticosteroids. As can be observed, at the end of follow-up, the use of tacrolimus tended to equal that of cyclosporine in immunosuppression, despite the predominance of the latter in the immunosuppressive regimens at the initiation of treatment. Azathioprine was administered very little and, surprisingly, 27.7% of the patients were being treated with mTOR inhibitors (everolimus or sirolimus) at the last follow-up.
. Variations according to type of drug: at start of transplantation and at the end of follow-up. MMF, mycophenolate mofetil; MPS, mycophenolate sodium.")
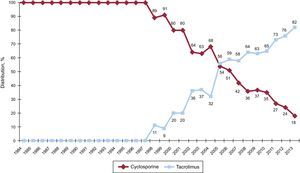
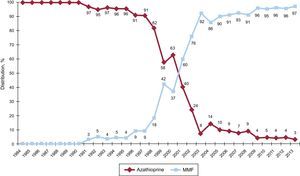
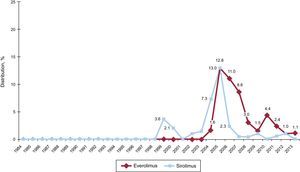
The changes from one year to another in the use of the different calcineurin inhibitors and antimycotic agents are shown in Figures 7 and 8, respectively. The use of tacrolimus equalled that of cyclosporine in 2005 and, since then, continued to exhibit an upward trend to ultimately become the predominant calcineurin inhibitor in initial immunosuppression. A similar trend was observed between mycophenolate mofetil and azathioprine, the use of which be came equalled between 1999 and 2001; mycophenolate mofetil became the predominant antimycotic agent in initial immunosuppression, relegating azathioprine to minimal use from 2009 on. The changes over time in the use of mTOR inhibitors (sirolimus, everolimus) in initial immunosuppression are illustrated in Figure 9. These drugs were initially used in a considerable number of cases in 2005-2007, but their use subsequently fell to minimum levels.
 in initial immunosuppression in the overall sample (1984-2013).")
 in initial immunosuppression in the overall sample (1984-2013). MMF, mycophenolate mofetil.")
 in initial immunosuppression in the overall sample (1984-2013).")
Figure 10 shows the changes over the years in the operative mortality (within 30 days of transplantation). In 2013, it was 11.3%, slightly lower than that of the historical cohort, in which the annual average was 15%.
. Early mortality does not include early graft loss.")
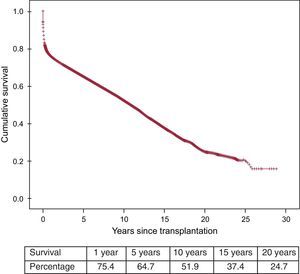
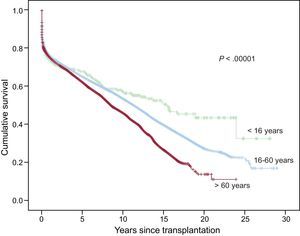
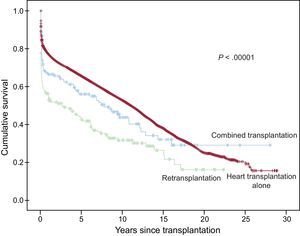
In the most recent update, dated 31 December 2013, the actuarial survivals at 1, 5, 10, 15, and 20 years in the entire time series are shown in Figure 11. This represents a mean annual mortality of approximately 2% to 3%, with a median survival of 10.8 years. There were significant differences depending on the age of the recipient at the time of transplantation and the type of procedure. The rate of survival of the patients < 16 years was significantly higher than that of patients aged 16 to 60 years, as was that of the latter group with respect to patients > 60 years of age (Figure 12). There were also highly significant differences between patients receiving a cardiac graft alone, those undergoing heart transplantation combined with kidney, liver, or lung transplantation, and cases of retransplantation (Figure 13).

.")

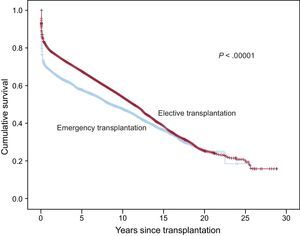
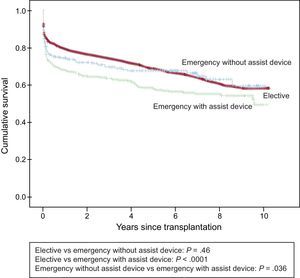
The examination of the entire time series revealed highly significant differences between elective and emergency transplantation (Figure 14). Analysis of the period from 2004 to 2013, during which the use of mechanical assist devices increased considerably, survival in elective transplantation was not significantly different from that of emergency transplantation performed with the support of inotropic drugs alone or, in most cases, with intraaortic balloon counterpulsation (P=.46), but was significantly higher than the survival in emergency transplantation with mechanical assistance (P<.0001) (Figure 15). The survival rate was also significantly higher in emergency transplantation with balloon counterpulsation (P=.036) than in emergency transplantation performed after the use of ventricular assist devices (Figure 15).


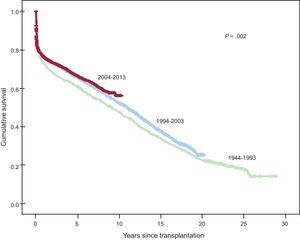
Beyond the first decade (1984-1993), there was a significant improvement in medium- and long-term survival, due mainly to the lower mortality rate during the early stages following transplantation (Figure 16). Over the past decade (2004-2013), with respect to the immediately preceding decade (1994-2003), we observe a nonsignificant trend toward an improvement in survival starting the fifth year after transplantation (Figure 16).
Causes of Death.")
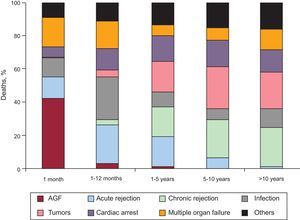
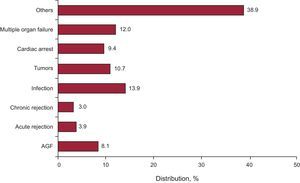
The causes of death changed according to the post-transplantation period under consideration (Figure 17). In the first month after transplantation, nearly 50% of the deaths were due to primary graft failure. After the first month, and up to the end of the first year, acute rejection and, above all, infections were the main causes of death. After the first year, the major causes were tumors and the different manifestations of graft vascular disease (chronic rejection, sudden cardiac death). Figure 18 shows the major causes of death in the entire time series. Overall, they were infection (13.9%), conditions mainly attributable to graft vascular disease (chronic rejection, sudden cardiac death) (12.4%), multiple organ failure (12%), and tumors (9.4%). Only 3.9% of all the deaths were due to acute rejection.

. AGF, acute graft failure.")
Heart transplantation is currently a well-established therapy for patients with advanced heart disease for whom there is no other reasonable therapeutic alternative. This year commemorates the 30th anniversary of the performance of the first viable heart transplantation in Spain. For its part, the RETC now marks 25 years of activity, which began in 1989, and they published their first report in 1991.1 The collaborative effort of all the Spanish heart transplantation groups ensuring the comprehensive nature of the RETC, with the inclusion of all the patients who underwent transplantation in Spain and with nearly nonexistent losses to follow-up, permits a consistent overview of this procedure, placed in the perspective of our population from the initiation of transplantation activity in Spain. Prospective and standardized data collection, and with a dynamic adaptation to the historical course of the procedure, proves to be a research instrument and, above all, a clinical tool of the greatest importance. This is particularly true in cases like heart transplantation in Spain, a procedure that is performed in nearly all the regions of Spain (at the present time, there are programs in 18 centers) and, consequently, the volume per center is low. It seems obvious that only the analysis of the data on a nationwide basis can ensure a minimum of consistency in the findings. Nevertheless, an in-depth analysis that explains the historical trends in heart transplantation in Spain is not always possible on the part of the RETC since this registry lacks certain important data, such as the number of patients on the waiting list or the time spent on the waiting list before the transplantation is performed.
In 2013, 248 transplantations were carried out, a number that is similar to that of previous years. This fact confirms the decrease in the number of procedures observed after the peak reached in the late nineties, a finding that is common throughout Europe.25 In contrast, this year there has been a significant increase in pediatric transplantation, a circumstance that may reflect the progressive maturing and revitalization of pediatric transplantation programs in Spain.
The characteristics of the procedures performed in 2013 confirm the trends observed in previous years24 and largely reflect a change in the paradigm of the treatment of advanced heart failure. Primarily, our data show a progressive deterioration of the clinical profile of the recipient. In the last 5 to 10 years, there is a higher percentage of older patients, with worse renal function, a higher prevalence of insulin-dependent diabetes mellitus, and a more widespread use of mechanical ventilation, factors that are all known to have an influence on the short- and long-term prognosis.25 It is possible to detect a progressive expansion of the criteria for donation, as seems to be reflected in the significant increase in the mean age of the donors and the percentage of older donors (> 45 years of age), as well as the number of donors in whom the cause of death was stroke, frequently associated with a higher incidence of arteriosclerosis. In the third place, there is a notable increase in the number of emergency transplantations and, above all, with circulatory assist devices (extracorporeal membrane oxygenation, mechanical ventricular assistance), which now correspond to half of the emergency transplantations and equal those carried out with balloon counterpulsation. Undoubtedly, this is possible due to the growing availability of these devices in the advanced heart failure units that perform the transplantation and is in accordance with the general trend observed in developed countries.26 These devices enable the optimization of the patient for transplantation in acute situations of utmost emergency (massive acute myocardial infarction, cardiogenic shock, postcardiotomy shock) and the stabilization of the end-stage patient with a long history of disease and very severe and irreversible deterioration.27 As we predicted in the RETC report published in 2013, the expansion of the use of circulatory assist devices has changed the criteria for inclusion on the waiting list for emergency transplantation in Spain, and their effectiveness will need to be evaluated in the coming years. Finally, this new clinical scenario explains the significant prolongation of the ischemia times, another factor that has a marked impact on prognosis in heart transplantation, and is very probably a consequence of the acceptance of grafts from geographically distant areas and a more complex and sometimes less predictable surgical procedure.
The time-scale changes in immunosuppression are equally notable. There has been a generalization of the administration of induction therapy with antibodies, especially interleukin 2 inhibitors, which allow the delay of the introduction of calcineurin inhibitors, an increasingly common strategy in situations of perioperative renal failure. The clinical tolerance to these agents is much greater than that observed with now obsolete drugs like OKT3. Currently, initial immunosuppression continues to be based on the traditional triple therapy, although there has been a definite change in the choice of calcineurin inhibitors favoring tacrolimus and in that of antiproliferative agents favoring mycophenolate mofetil, rather than cyclosporine and azathioprine, respectively. The expectations generated by the introduction of mTOR inhibitors (sirolimus and everolimus) led to the wide use of these drugs as initial therapy around 2005. This use declined soon after once the complexity of their utilization in de novo heart transplantation had been confirmed. However, they are an established therapeutic option during the chronic phase of transplantation, as shown by the fact that, an average of 7 years after transplantation, these drugs are included in the immunosuppressive regimens of more than 25% of our patients.
Despite the progressive complication of the clinical scenario in which heart transplantation is currently being performed, the results in terms of mortality have remained stable over the past 20 years. These results are comparable to those reported in the registry of the International Society for Heart and Lung Transplantation.25 After the initial period (1984-1993), there was a significant improvement in survival, due mainly to the reduction of the mortality during the first year after transplantation and, subsequently, the long-term curves remained parallel. Since 1994, early survival has remained stable, although a trend toward an improvement in survival is observed from the fifth year on during the period from 2004 to 2013 with respect to the period from 1994 to 2003. A longer-term observation will enable us to determine whether this improvement is significant and could perhaps lead to a better management of the patient over the long term, largely due to refinements in the immunosuppressive therapies. It is notable that in 2013, despite the considerable increase in emergency procedures, there has been a decrease in early mortality (first 30 days), which began to be detected in 2012. The expansion of the utilization of circulatory assist devices in these cases could be one of the causes of this finding,27 a possibility that will need to be confirmed in coming years.
In the analysis of the causes of death in the entire time series, it appears evident that acute rejection, the risk of which does not disappear at any time during the post-transplantation course, is now a clinically controlled condition. In contrast, the predominant causes of death include infections, tumors, multiple organ failure (largely mediated by the incidence of chronic kidney disease) and manifestations characteristic of graft vascular disease. These conditions are related etiologically and pathogenically to the effects of the immunosuppressive medication. The changes recently produced in immunosuppression, which make it possible to minimize it and, up to a certain point, individualize it, could have a marked influence on the long-term prognosis of our patients.
CONCLUSIONSIn 30 years of experience with heart transplantation in Spain, this strategy has become a fully developed procedure with a well-established indication for the treatment of advanced heart failure. Despite the deterioration and the complications of the current clinical context, the Spanish groups have achieved stability in the results, and their are well founded reasons to expect these results to improve with the refinement in the use of circulatory assist devices and immunosuppressive regimens.
FUNDINGThe RETC is partly funded by an unconditional grant from Novartis.
CONFLICTS OF INTERESTF. González-Vílchez is being remunerated by Roche and Astellas for participating in the committee of control and statistical analysis and by Roche, Astellas, and Novartis for giving talks and educational presentations and for travel expenses. M.G. Crespo-Leiro is being remunerated by Roche, Astellas, and Novartis for giving talks and educational presentations and for travel expenses.
We thank ODDS, SL, for their help with the statistical analysis.
| Clínica Universitaria Puerta de Hierro, Majadahonda, Madrid | Javier Segovia-Cubero, Inés Sayado, and Luis Alonso-Pulpón |
| Hospital Universitario y Politécnico La Fe, Valencia | Luis Martínez-Dolz, Ignacio Sánchez-Lázaro, and Mónica Cebrián |
| Hospital Universitario de A Coruña, A Coruña | Maria J. Paniagua-Martin, Raquel Marzoa-Rivas, and Eduardo Barge-Caballero |
| Hospital Universitario Reina Sofía, Córdoba | Amador Lopez-Granados and Juan Carlos Castillo-Dieguez |
| Hospital Universitario Marqués de Valdecilla, Santander | Miguel Llano-Cardenal and Jose A. Vázquez de Prada |
| Hospital Gregorio Marañón (adults), Madrid | Adolfo Villa, Juan Fernández-Yáñez, Iago Sousa, and Pablo Díez |
| Hospital Universitario 12 de Octubre, Madrid | Maria J. Ruiz, Pilar Escribano, Miguel A. Gómez, and Marta Paradina |
| Hospital de la Santa Creu i Sant Pau, Barcelona | Vicenç Brosa, Sonia Mirabet, Laura López, and Josep Padró |
| Hospital Universitario Virgen del Rocío, Sevilla | Jose Manuel Sobrino and Alejandro Adsuar |
| Hospital Universitario de Bellvitge, L’Hospitalet de Llobregat, Barcelona | Josep Roca-Elías, José González-Costello, and Joel Salazar-Mendiguchía |
| Clínica Universitaria de Navarra, Pamplona | Beltrán Levy and Rafael Hernández |
| Hospital Clínic Universitari, Barcelona | Marta Farrero and M. Ángeles Castel |
| Hospital Universitario Central de Asturias, Oviedo | Beatriz Díez de Molina |
| Hospital Universitario Gregorio Marañón (children), Madrid | Constancio Medrano |
| Hospital Universitario Virgen de la Arrixaca, El Palmar, Murcia | Iris Garrido |
| Hospital Universitario Miguel Servet, Zaragoza | María L. Sanz-Julvé |
| Hospital Clínico Universitario, Valladolid | Javier López-Díaz and Amada Recio |
| Hospital Universitario La Paz, Madrid | Daniel Borches, Luz Polo, Carlos Labrandero, and Lucía Deiros |
| Hospital Universitario Vall d’Hebron, Barcelona | Ferrán Gran and Raúl Abella |