The present report updates the characteristics and results of heart transplantation in Spain, mainly focused in the 2008-2017 period.
MethodsWe describe the recipient and donor characteristics, surgical procedures, and outcomes of heart transplants performed in 2017. The 2017 data were compared with those obtained from 2008 to 2016.
ResultsA total of 304 cardiac transplants were performed in 2017. Between 1984 and 2017, 8173 procedures were performed, 2689 of them after 2008. Significant temporal trends were observed in recipient characteristics (lower pulmonary vascular resistance, lower use of mechanical ventilation, and a higher percentage of diabetic patients and those with previous cardiac surgery), donor characteristics (older donor age and a higher percentage of female donors and those with a prior cardiac arrest) and procedures (lower ischemia time). In 2017, 27% of patients were transplanted after undergoing mechanical ventricular assistance (P <.001 for trend). In the last decade, there was a trend to better survival.
ConclusionsAround 300 transplants per year were performed in Spain in the last decade. There was a significant increase in the use of pretransplant mechanical circulatory support and a trend to improved survival.
Keywords
In the absence of contraindications, heart transplant is currently the recommended treatment for heart failure patients whose condition remains critical despite optimal medical and device therapy. In 2016, more than 7000 heart transplant procedures were performed worldwide, with more than a third of them in Europe.1 For low prevalence diseases and procedures such as heart transplant, one of the most effective ways to improve quality of care and clinical research is to maintain a clinical registry. These registries are especially valuable if they are comprehensive, like the Spanish Heart Transplant Registry (Registro Español de Trasplante Cardiaco [RETC]).
This annual report provides an update on the RETC, incorporating transplant data from 2017.
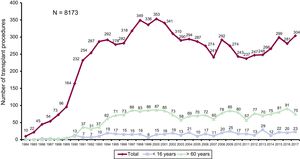
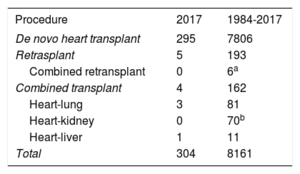
METHODSPatients and ProceduresThe data analyzed cover the clinical characteristics of recipients and donors, surgical procedures, immunosuppression, and mortality in the 18 active heart transplant programs in Spain (Table 1). Of the participating centers, 6 carry out pediatric heart transplants, 2 of them exclusively, and 2 of the centers carry out combined heart-lung transplants. The numbers of procedures performed since the first use of this therapeutic modality are summarized in Figure 1. Since 1984, 8173 heart transplant procedures have been carried out in Spain. The types of procedures performed in the whole series are summarized in Table 2.
Centers Participating in the Spanish Heart Transplant Registry by Order of First Transplant Performed (1984-2017)
| 1. Hospital de la Santa Creu i Sant Pau, Barcelona |
| 2. Clínica Universitaria de Navarra, Pamplona |
| 3. Hospital Universitario Puerta de Hierro-Majadahonda, Majadahonda, Madrid |
| 4. Hospital Marqués de Valdecilla, Santander |
| 5. Hospital Reina Sofía, Córdoba (adults and pediatric) |
| 6. Hospital Universitario y Politécnico La Fe, Valencia (adults and pediatric) |
| 7. Hospital Gregorio Marañón, Madrid (adults and pediatric) |
| 8. Fundación Jiménez Díaz, Madrid (1989-1994) |
| 9. Hospital Virgen del Rocío, Seville |
| 10. Hospital 12 de Octubre, Madrid |
| 11. Hospital Universitario de A Coruña, La Coruña (adults and pediatric) |
| 12. Hospital Bellvitge, L’Hospitalet de Llobregat, Barcelona |
| 13. Hospital La Paz, Madrid (pediatric) |
| 14. Hospital Central de Asturias, Oviedo, Asturias |
| 15. Hospital Clínic, Barcelona |
| 16. Hospital Virgen de la Arrixaca, El Palmar, Murcia |
| 17. Hospital Miguel Servet, Zaragoza |
| 18. Hospital Clínico, Valladolid |
| 19. Hospital Vall d’Hebron, Barcelona (pediatric) |
, in the total series and by age group.")
The present report analyzes results from the past 10 years (2008-2017). To analyze time trends, most results were grouped into 3-year transplant periods (2008-2010, 2011-2013, and 2014-2016). The percentage of urgent transplants, the type of circulatory support, and donor age were analyzed by year of transplant.
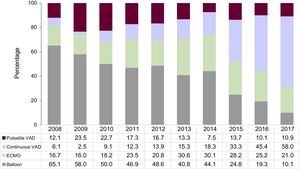
The database structure and RETC practices concerning data collection, data handling, auditing, and data protection have been described previously.2 An effort has been made to present statistical data from before 2017 in a format consistent with previous studies; however, the process of continually updating the registry database may have led to the introduction of minor discrepancies in decimals. Nevertheless, any such minor discrepancies do not significantly affect the trends in proportions shown with this same updating procedure, which reveals large changes in pretransplant circulatory support (Figure 2).
Statistical Analysis. ECMO, extracorporeal membrane oxygenation; VAD, ventricular assist device.")
Continuous variables are expressed as mean±standard deviation, and categorical variables as as percentages. Between-group differences in categorical variables were analyzed by the Kendall tau nonparametric test for a time series trend, whereas between-group differences in continuous variables were examined by analysis of variance with polynomial adjustment. Survival curves were calculated using the Kaplan-Meier method and were compared by the log-rank test. Differences were considered statistically significant at P <.05.
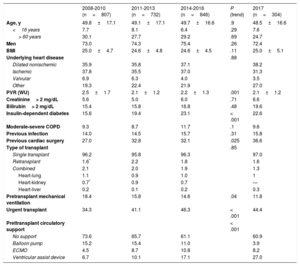
RESULTSRecipient CharacteristicsThe main recipient characteristics by 3-year transplant period are summarized in Table 3. In 2017, there were 304 transplant procedures, 23 (7.6%) of them in recipients younger than 16 years. Approximately 3 of every 4 recipients were men, and mean recipient age was 48.5 (range, 0.05-73.0) years. The mean age of adult recipients was 51.8 years. Most procedures were de novo heart-only transplants (97%), with retransplants and combined transplants accounting for less than 3% of the total. Most combined transplant procedures were heart and lung or heart and kidney. These rates have remained largely unaltered since 2008.
Recipient Characteristics in the Spanish Heart Transplant Registry (2008-2017)
| 2008-2010 (n=807) | 2011-2013 (n=732) | 2014-2016 (n=846) | P (trend) | 2017 (n=304) | |
|---|---|---|---|---|---|
| Age, y | 49.8±17.1 | 49.1±17.1 | 49.7±16.6 | .9 | 48.5±16.6 |
| <16 years | 7.7 | 8.1 | 6.4 | .29 | 7.6 |
| > 60 years | 30.1 | 27.7 | 29.2 | .69 | 24.7 |
| Men | 73.0 | 74.3 | 75.4 | .26 | 72.4 |
| BMI | 25.0±4.7 | 24.6±4.8 | 24.6±4.5 | .11 | 25.0±5.1 |
| Underlying heart disease | .88 | ||||
| Dilated nonischemic | 35.9 | 35.8 | 37.1 | 38.2 | |
| Ischemic | 37.8 | 35.5 | 37.0 | 31.3 | |
| Valvular | 6.9 | 6.3 | 4.0 | 3.5 | |
| Other | 19.3 | 22.4 | 21.9 | 27.0 | |
| PVR (WU) | 2.5±1.7 | 2.1±1.2 | 2.2±1.3 | .001 | 2.1±1.2 |
| Creatinine> 2 mg/dL | 5.6 | 5.0 | 6.0 | .71 | 6.6 |
| Bilirubin> 2 mg/dL | 15.4 | 15.8 | 16.8 | .48 | 19.6 |
| Insulin-dependent diabetes | 15.6 | 19.4 | 23.1 | < .001 | 22.6 |
| Moderate-severe COPD | 9.3 | 8.7 | 11.7 | .1 | 9.6 |
| Previous infection | 14.0 | 14.5 | 15.7 | .31 | 15.8 |
| Previous cardiac surgery | 27.0 | 32.8 | 32.1 | .025 | 36.6 |
| Type of transplant | .85 | ||||
| Single transplant | 96.2 | 95.8 | 96.3 | 97.0 | |
| Retransplant | 1.6* | 2.2 | 1.8 | 1.6 | |
| Combined | 2.1 | 2.0 | 1.9 | 1.3 | |
| Heart-lung | 1.1 | 0.9 | 1.0 | 1 | |
| Heart-kidney | 0.7* | 0.9 | 0.7 | — | |
| Heart-liver | 0.2 | 0.1 | 0.2 | 0.3 | |
| Pretransplant mechanical ventilation | 18.4 | 15.8 | 14.6 | .04 | 11.8 |
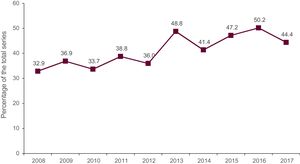
| Urgent transplant | 34.3 | 41.1 | 46.3 | < .001 | 44.4 |
| Prettransplant circulatory support | < .001 | ||||
| No support | 73.6 | 65.7 | 61.1 | 60.9 | |
| Balloon pump | 15.2 | 15.4 | 11.0 | 3.9 | |
| ECMO | 4.5 | 8.7 | 10.8 | 8.2 | |
| Ventricular assist device | 6.7 | 10.1 | 17.1 | 27.0 |
BMI, body mass index; COPD, chronic obstructive pulmonary disease; ECMO, extracorporeal membrane oxygenation; PVR, pulmonary vascular resistance.
Data are expressed as the percentage or the mean±standard deviation.
Since 2008, there have been statistically significant trends toward lower pulmonary resistance (P <.001), increased percentages of recipients with diabetes (P <.001) and a history of cardiac surgery before transplant (P <.025), and a lower percentage of recipients receiving mechanical ventilation at the time of transplant (P <.04). Over the same period, there was an appreciable but nonsignificant trend toward an increase in the number of recipients with obstructive pulmonary disease (P <.10).
In 2017, 44% of transplant procedures were urgent (Figure 3), and 39.1% of transplant recipients received pretransplant circulatory support. Compared with previous years, there was a higher use of continuous-flow ventricular assist devices, with a marked reduction in the use of balloon pump counterpulsation. There were no changes in the use of extracorporeal membrane oxygenation (ECMO) and pulsatile-flow ventricular assist devices (Figure 2).
Donor Characteristics and Ischemia Time.")
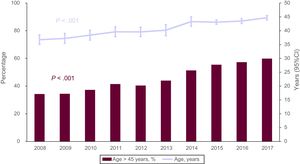
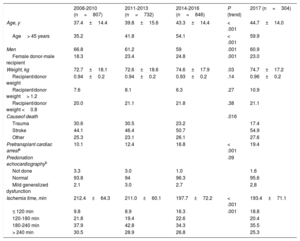
Donor characteristics for the 3-year transplant periods and for 2017 are summarized in Table 4. The trend toward a higher mean donor age continued in 2017, with donors older than 45 years now accounting for 60% of the total (Figure 4). There was a further increase in the percentage of donors who died due to stroke (54.9%), accompanied by corresponding decreases in the percentage who died due to trauma (17.4%) and in the number of donors with pretransplant cardiac arrest. In contrast, cold ischemia time decreased slightly in 2017, with a decrease in ischemia times >4hours (25.3%) and an increase in times <2hours.
Donor Characteristics and Ischemia Time in the Spanish Heart Transplant Registry (2008-2017)
| 2008-2010 (n=807) | 2011-2013 (n=732) | 2014-2016 (n=846) | P (trend) | 2017 (n=304) | |
|---|---|---|---|---|---|
| Age, y | 37.4±14.4 | 39.8±15.6 | 43.3±14.4 | < .001 | 44.7±14.0 |
| Age> 45 years | 35.2 | 41.8 | 54.1 | < .001 | 59.9 |
| Men | 66.8 | 61.2 | 59 | .001 | 60.9 |
| Female donor-male recipient | 18.3 | 23.4 | 24.8 | .001 | 23.0 |
| Weight, kg | 72.7±18.1 | 72.6±18.6 | 74.6±17.9 | .03 | 74.7±17.2 |
| Recipient/donor weight | 0.94±0.2 | 0.94±0.2 | 0.93±0.2 | .14 | 0.96±0.2 |
| Recipient/donor weight> 1.2 | 7.6 | 8.1 | 6.3 | .27 | 10.9 |
| Recipient/donor weight <0.8 | 20.0 | 21.1 | 21.8 | .38 | 21.1 |
| Causeof death | .016 | ||||
| Trauma | 30.6 | 30.5 | 23.2 | 17.4 | |
| Stroke | 44.1 | 46.4 | 50.7 | 54.9 | |
| Other | 25.3 | 23.1 | 26.1 | 27.6 | |
| Pretransplant cardiac arresta | 10.1 | 12.4 | 16.8 | < .001 | 19.4 |
| Predonation echocardiographyb | .09 | ||||
| Not done | 3.3 | 3.0 | 1.0 | 1.6 | |
| Normal | 93.8 | 94 | 96.3 | 95.6 | |
| Mild generalized dysfunction | 2.1 | 3.0 | 2.7 | 2.8 | |
| Ischemia time, min | 212.4±64.3 | 211.0±60.1 | 197.7±72.2 | < .001 | 193.4±71.1 |
| ≤ 120 min | 9.8 | 8.9 | 16.3 | .001 | 18.8 |
| 120-180 min | 21.8 | 19.4 | 22.6 | 20.4 | |
| 180-240 min | 37.9 | 42.8 | 34.3 | 35.5 | |
| > 240 min | 30.5 | 28.9 | 26.8 | 25.3 |
Data are expressed as the percentage or the mean±standard deviation.
. 95%CI, 95% confidence interval; ECMO, extracorporeal membrane oxygenation; VAD, ventricular assist device.")
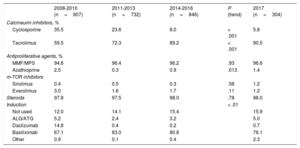
The drugs used for induction immunosuppression during the study period are summarized in Table 5. As in previous years, induction therapy in 2017 mostly consisted of tacrolimus (90.5%), mycophenolate (and to a much lower extent mycophenolic acid) (96.6%), and steroids (98%). Approximately 85% of transplant recipients in 2017 also received antibody-based induction therapy, mostly basiliximab (76.1%).
Induction Immunosuppression in the Spanish Heart Transplant Registry (2008-2017)
| 2008-2010 (n=807) | 2011-2013 (n=732) | 2014-2016 (n=846) | P (trend) | 2017 (n=304) | |
|---|---|---|---|---|---|
| Calcineurin inhibitors, % | |||||
| Cyclosporine | 35.5 | 23.6 | 8.0 | < .001 | 5.8 |
| Tacrolimus | 59.5 | 72.3 | 89.2 | < .001 | 90.5 |
| Antiproliferative agents, % | |||||
| MMF/MPS | 94.6 | 96.4 | 96.2 | .93 | 96.6 |
| Azathioprine | 2.5 | 0.3 | 0.9 | .013 | 1.4 |
| m-TOR inhibitors | |||||
| Sirolimus | 0.4 | 0.5 | 0.3 | .58 | 1.2 |
| Everolimus | 3.0 | 1.6 | 1.7 | .11 | 1.2 |
| Steroids | 97.8 | 97.5 | 98.0 | .78 | 98.0 |
| Induction | < .01 | ||||
| Not used | 12.0 | 14.1 | 15.4 | 15.9 | |
| ALG/ATG | 5.2 | 2.4 | 3.2 | 5.0 | |
| Daclizumab | 14.8 | 0.4 | 0.2 | 0.7 | |
| Basiliximab | 67.1 | 83.0 | 80.8 | 76.1 | |
| Other | 0.9 | 0.1 | 0.4 | 2.3 | |
ALG, antilymphocyte globulin; ATG, antithymocyte globulin, MMF, mycophenolate mofetil; MPS, mycophenolate sodium.
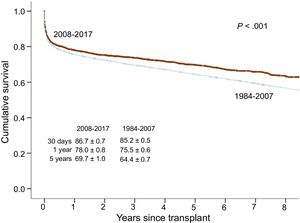
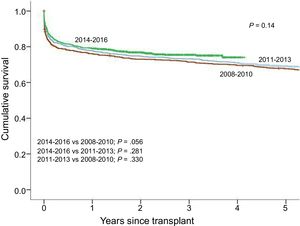
Recipient survival in the 2008 to 2017 and 1984 to 2007 periods is compared in Figure 5. Compared with the earlier period, the 2008 to 2017 period showed a statistically significant improvement in survival, attributable to increased survival rates both at 1 year and over the longer term. The 1-year survival rate showed a mean improvement of 2.5%. Beyond the first year, the yearly death rate decreased from 2.2% to 1.6%. This trend toward improved survival continued within the 2008 to 2017 study period, approaching significance (P <.056) for the comparison between the 2014 to 2016 and 2008 to 2011 3-year transplant periods (Figure 6).


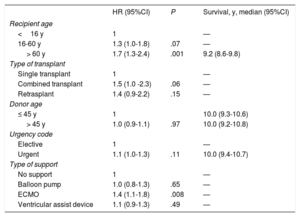
The dominant variables influencing survival during the study period were recipient age and the type of pretransplant circulatory support (Table 6). Compared with pediatric recipients (< 16 years old), recipients older than 60 years at the time of transplant had a 70% higher mortality risk (P <.001), whereas the increased risk in recipients between the ages of 16 and 60 years was > 30% (P <.07). Previous ECMO increased the mortality risk by more than 40% (P <.008) compared with patients with no circulatory support device. However, results for recipients with a balloon pump or ventricular assist device were indistinguishable from those of patients with no support device (Table 6). During the 2008 to 2017 study period, there was no evidence that survival was influenced by donor age or urgent vs elective transplant.
Univariate Survival Analysis by Baseline Characteristics of the Recipient, Donor, and Procedure (2008-2017)
| HR (95%CI) | P | Survival, y, median (95%CI) | |
|---|---|---|---|
| Recipient age | |||
| <16 y | 1 | — | |
| 16-60 y | 1.3 (1.0-1.8) | .07 | — |
| > 60 y | 1.7 (1.3-2.4) | .001 | 9.2 (8.6-9.8) |
| Type of transplant | |||
| Single transplant | 1 | — | |
| Combined transplant | 1.5 (1.0 -2.3) | .06 | — |
| Retrasplant | 1.4 (0.9-2.2) | .15 | — |
| Donor age | |||
| ≤ 45 y | 1 | 10.0 (9.3-10.6) | |
| > 45 y | 1.0 (0.9-1.1) | .97 | 10.0 (9.2-10.8) |
| Urgency code | |||
| Elective | 1 | — | |
| Urgent | 1.1 (1.0-1.3) | .11 | 10.0 (9.4-10.7) |
| Type of support | |||
| No support | 1 | — | |
| Balloon pump | 1.0 (0.8-1.3) | .65 | — |
| ECMO | 1.4 (1.1-1.8) | .008 | — |
| Ventricular assist device | 1.1 (0.9-1.3) | .49 | — |
95%CI, 95% confidence interval; ECMO, extracorporeal membrane oxygenation; HR, hazard ratio.
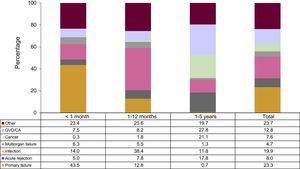
During the study period, the principal cause of death in the first posttransplant year was primary graft failure (32.6%), especially in the first month (43.5%), followed by infection (22.9%). Between the first and fifth posttransplant years, the most frequent causes of death were graft vascular disease/cardiac arrest (27.8%) and cancer (21.1%) (Figure 7). Overall, acute rejection caused 8% of posttransplant deaths, with the rate almost 3-fold higher (17.8%) between the first and fifth posttransplant years than in the first year (6.1%).

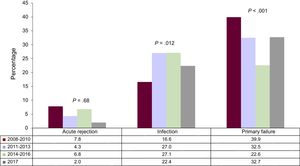
Almost all patients included in the present analysis survived the first year after transplant. Among those who did not, infection increased significantly as the cause of death between the 2008 to 2010 and 2011 to 2013 transplant periods, thereafter remaining stable (Figure 8). In contrast, primary graft failure showed a progressive and statistically significant decline as the cause of death in the first posttransplant year. Mortality due to transplant rejection has remained stable over the last decade (Figure 8).
 by 3-year period. P values indicate the significance of the trend between 3-year periods, excluding 2017. Only 17 patients receiving a heart transplant in 2017 had completed ≥ 1-year follow-up at the time of database closure.")
Main causes of death occurring in the first year after transplant (2008-2016) by 3-year period. P values indicate the significance of the trend between 3-year periods, excluding 2017. Only 17 patients receiving a heart transplant in 2017 had completed ≥ 1-year follow-up at the time of database closure.
Heart transplant activity in Spain has remained steady in recent years, at approximately 250 to 300 transplants a year. Given current donor characteristics and the exclusive sourcing of hearts from brain-dead donors, these figures are likely very close to the upper limit for heart transplant in Spain. Relaxation of the criteria for donor hearts, especially to allow donation after circulatory death, could increase organ supply, as demonstrated in small-scale studies in other countries.3 Organ supply could also be increased by routine use of coronary angiography in older donors or those with cardiovascular risk factors, who currently constitute the majority of heart donors in Spain.4
The data from 2017 confirm and in some instances reinforce the trends observed over the past decade. In addition to the increasing use of older donors who until recently would have been considered “borderline”, perhaps the most remarkable finding is the change in the type of circulatory support at the time of urgent intervention. The previous RETC report already revealed the worse short-term survival among recipients supported by ECMO than among those with ventricular assist devices.2 These findings were recently confirmed by a more comprehensive analysis of the RETC data5 and form the basis for the recent adjustment of the urgency code criteria, introduced by the Organización Nacional de Trasplantes (Spanish National Transplant Organization) in June 2017. Clinical stabilization with ventricular assist devices maintains the recipient in a better medical and hemodynamic condition during the transplant procedure, thus reducing the need for mechanical ventilation.6,7 Using this approach, it is possible to achieve survival levels similar to those obtained after elective transplant.
The current data maintain the trend toward improved outcomes seen in previous reports. This trend did not reach statistical significance, probably due to the small sample size; nonetheless, the trend is apparent even over the past 10 years. The most notable development has been the reduction in early posttransplant mortality. This has been achieved largely through the progressive decline in deaths due to primary graft failure, as well as the stabilization of mortality due to infection and acute rejection. The declining rate of primary graft failure can be explained by improved prevention due to the decline in mean ischemia time, in combination with improved therapy through the broad implementation of circulatory support programs, which are especially effective for the treatment of this serious complication.8
CONCLUSIONSHeart transplant activity in Spain has stabilized at approximately 250 to 300 procedures per year. In 2017, there was an increase in the prettransplant use of ventricular assist devices and a continuation of the trend to use organs from older donors. Recipient survival continued to show a trend toward progressive improvement.
CONFLICTS OF INTERESTF. González-Vílchez has participated in Novartis educational presentations and has received compensation for travel costs from Pfizer and Bayer. M.G. Crespo-Leiro is the recipient of a CIBERCV grant, has participated in educational presentations for Novartis, Astellas, MSD, and Abbott, and has received compensation for travel costs from Novartis and Astellas. J. González-Costelo acts as a consultant for Alnylam, Abbot, Pfizer, and Novartis, has delivered lectures for Novartis, and has received compensation for travel costs from Astellas and Servier.
| Hospital Universitario Puerta de Hierro-Majadahonda, Majadahonda, Madrid | Javier Segovia-Cubero, Manuel Gómez-Bueno, Francisco Hernández-Pérez |
| Hospital Universitario y Politécnico La Fe, Valencia | Soledad Martínez-Penades, Mónica Cebrián-Pinar, Raquel López-Vilella, Ignacio Sánchez-Lázaro, Luis Martínez-Dolz |
| Complejo Hospitalario Universitario de A Coruña, A Coruña | María J Paniagua-Martín, Eduardo Barge-Caballero, Gonzalo Barge-Caballero, David Couto-Mallón |
| Hospital Universitario Reina Sofía, Córdoba | Amador López-Granados, Carmen Segura-Saintgerons, Dolores Mesa, Martín Ruiz, Elías Romo, Francisco Carrasco, José López-Aguilera |
| Hospital Universitario Marqués de Valdecilla, Santander | Manuel Cobo, Miguel Llano-Cardenal, José A. Vázquez de Prada, Francisco Nistal-Herrera |
| Hospital Gregorio Marañón (adults), Madrid | María Jesús Valero, Juan Fernández-Yáñez, Paula Navas, Carlos Ortiz, Adolfo Villa, Eduardo Zataraín, Manuel Martínez-Sellés |
| Hospital Universitario 12 de Octubre, Madrid | María Dolores García-Cosío, Laura Morán-Fernández, Zorba Blázquez |
| Hospital de la Santa Creu i Sant Pau, Barcelona | Eulàlia Roig-Minguell, Vicens Brossa-Loidi, Sonia Mirabet-Pérez, Laura López-López |
| Hospital Universitario Virgen del Rocío, Sevilla | Ernesto Lage-Gallé, Diego Rangel-Sousa |
| Hospital Universitario de Bellvitge, L’Hospitalet de Llobregat, Barcelona | Nicolás Manito-Lorite, Carles Díez-López, Josep Roca-Elías |
| Clínica Universitaria de Navarra, Pamplona | Gregorio Rábago-Aracil |
| Hospital Clínic Universitari, Barcelona | María Ángeles Castel, Marta Farrero, Ana García-Álvarez |
| Hospital Universitario Central de Asturias, Oviedo | José Luis Lambert-Rodríguez, Beatriz Díaz-Molina, María José Bernardo-Rodríguez |
| Hospital Universitario Gregorio Marañón (pediatric), Madrid | Manuela Camino-López, Juan Miguel Gil-Jaurena, Nuria Gil-Villanueva |
| Hospital Universitario Virgen de la Arrixaca, El Palmar, Murcia | Iris Garrido-Bravo |
| Hospital Universitario Miguel Servet, Zaragoza | Teresa Blasco-Peiró, Ana Pórtoles-Ocampo, Marisa Sanz-Julve |
| Clínico Universitario, Valladolid | Luis de la Fuente-Galán, Javier Tobar-Ruiz, Ana María Correa-Fernández |
| Hospital Universitario La Paz, Madrid | Luis García-Guereta Silva, Álvaro González-Rocafort, Carlos Labradero-de Lera, Luz Polo- López |
| Hospital Universitario Vall d’Hebron, Barcelona | Dimpna C. Albert-Brotons, Ferrán Gran-Ipiña, Raúl Abella-Antón |
.