To the Editor:
Prinzmetal or variant angina, described for the first time half a century ago,1 is a rare cause of myocardial ischemia. The pathophysiological basis of this condition is reversible coronary spasm that usually appears at rest and, therefore, presentation as multivessel coronary spasm is rare.
We describe a 56-year-old woman recently diagnosed with hypertension. Chlorthalidone therapy was started, with control of blood pressure values. While the patient was taking a walk, she presented mid-chest pain and sudden syncope from which she recovered spontaneously, only to lose consciousness a few minutes later. She was seen by outpatient services, which found her recovered, hemodynamically stable, and with normal sinus rhythm during monitoring.
The patient was transferred to our hospital where a prolonged QTc interval and hypopotassemia (2.6 mEq/L) were detected in the physical examination and other initial tests. Based on suspected hypopotassemia secondary to diuretic therapy and syncope probably related to torsade de pointes, the patient was admitted for monitoring and potassium replacement.
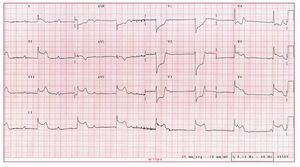
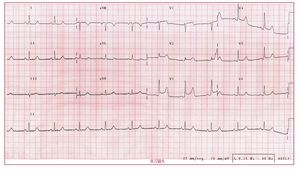
She remained asymptomatic for 36 hours, and the serum potassium values and electrocardiogram returned to normal. She experienced another syncopal episode, preceded by mid-chest pain. Electrocardiography revealed sinus rhythm with complete atrioventricular block and escape rhythm, narrow QRS, ST segment elevation at II, III, aVF, V5, V6, and aVL, and depression at V1 to V3 (Figure 1). Before any treatment could be given, the patient regained consciousness and atrioventricular conduction, and showed a virtually normal electrocardiogram. After only a few minutes, she complained of a new episode of chest pain. In this case, the monitor showed sinus rhythm with normal atrioventricular conduction, although the electrocardiogram revealed a new ST segment elevation, but at V1 to V4, the only ones not elevated during the episode a few minutes earlier (Figure 2). Coronary spasm was suspected to be the primary cause and sublingual nitroglycerin was started, followed by intravenous perfusion of diltiazem, which controlled the patient's symptoms.

Figure 1. Complete atrioventricular block with inferoposterolateral ST segment elevation.

Figure 2. Normal atrioventricular conduction with anterior ST segment elevation.
Coronary angiography 48 hours later showed normal coronary vasculature and no angiographic lesions. Given the typical symptoms, an ergonovine test was considered unnecessary. The patient remained asymptomatic for the remainder of her hospitalization and was discharged with 240 mg of diltiazem per day. Six months later, there was no evidence of symptom recurrence.
In recent series, Prinzmetal or variant angina was considered the cause of myocardial ischemia in 1.5% of patients with suspected coronary disease.2 The presentation as multivessel coronary spasm varies in frequency according to the diagnostic method used, ranging from 5.6% to 45%,2,3 with an incidence as high as 75% when coronary angiography is performed with pharmacological induction.4 Various patterns have been described3: a) migratory spasm affecting different sites on different occasions; b) sequential spasms successively affecting different sites; and c) simultaneous spasm occurring at different sites. Multivessel coronary spasm is known to have a poorer prognosis than single-site Prinzmetal angina, although patients with sequential or simultaneous spasm appear to have poorer prognosis in multivessel coronary spasm than those with migratory coronary spasm.5
The case we describe is notable because of its clinical presentation as syncope preceded by chest pain, which we attributed to and later found to be complete atrioventricular block. However, even more striking is the sequence of subsequent events, in which multiple coronary arteries (presumably the right coronary and left anterior descending arteries) experienced spasm only a few minutes apart between the different vascular territories. The symptoms can be classified as Prinzmetal or variant angina with sequential multivessel coronary spasm.