To the Editor,
Rotational atherectomy (RA) is a useful technique in calcified and diffuse lesions. Drug-eluting stents make it possible to treat long lesions and, thus, the use of RA has increased.1 However, the gauge of the catheters employed in radial access limits the utilization of RA. We describe the use of a 7.5-Fr catheter with a 0.081-inch lumen, designed for radial access, that enables the use of burrs measuring 2mm or less and allows revascularization immediately after coronary angiography when carried out using a radial approach and when a 1.75-mm or 2-mm burr is required.
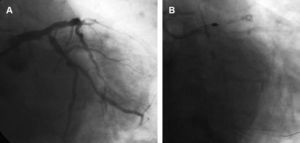
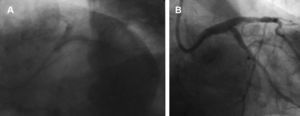
Four patients with stable angina underwent coronary angiography via right radial artery with a 6-Fr catheter and 5000 IU of sodium heparin. In all four patients, we found a highly calcified lesion in a vessel larger than 3mm, and revascularization during the same procedure was indicated. Three of the lesions treated were located in mid left anterior descending coronary artery, at the origin of the first diagonal branch and at the origin of the circumflex artery; the fourth was a long lesion in proximal and mid right coronary artery. Due to the marked calcification and the diameter of the vessel, RA with a burr diameter greater than or equal to 1.75mm was indicated and the 7.5-Fr Sheathless Eaucath® catheter (Asahi Intecc, Japan) was chosen. Once the heparin dose had been administered, the radial introducer sheath was withdrawn over the 280-cm-long 0.035-inch guiding catheter and the catheter was advanced with its guidewire in the interior. Previously, the catheter had been prepared by introducing the guidewire to the extreme end and maintaining it in that position for 3 to 4 min, in accordance with the recommendation of the manufacturer. At the level of ascending aorta, we began to withdraw the guidewire and the 0.035-inch guiding catheter, and the catheter was introduced into the coronary artery. In two of the cases, we employed a 1.75-mm burr and in the other two, we used a 1.75-mm burr followed by a 2-mm burr prior to balloon dilatation and implantation of the stent. All patients were discharged from the hospital the next day without complications. Figure 1, Figure 2 illustrate a procedure carried out at the origin of the circumflex artery using 1.75-mm and 2-mm burrs, followed by T stenting with a 3.5-mm×13-mm Cypher stent and implantation of another 3.5-mm×23-mm Cypher stent extending from left main coronary artery to anterior descending coronary artery. The procedure was completed with final kissing balloon technique with 3.5-mm and 4-mm balloons.

Figure 1. A: 7.5-Fr 3.5 SPB catheter and lesion at the origin of the circumflex artery. B: Ablation with 1.75-mm and 2-mm burrs.

Figure 2. A: Kissing balloon technique following implantation of a 3.5-mm×13-mm Cypher stent in the origin of the circumflex artery and a second one, measuring 3.5mm×23mm, extending from left main coronary artery toward anterior descending coronary artery. B: Final result.
The Asahi 7.5-Fr Sheathless Eaucath® catheter has no introducer sheath and its outer diameter is 2.49mm, smaller than the 2.62mm of the 6-Fr introducer sheath. It has an outer hydrophilic coating that facilitates its smooth passage and reduces the possibility of spasm. It provides an inner lumen of 0.081 inches and enables the performance of RA with burrs measuring 2mm or less. In contrast to standard catheters that have a single layer of metallic braiding, the wall of this catheter is thicker as it has an additional layer of braiding and the outer hydrophilic coating. There is now a second version, which constitutes an improvement over the first. On one hand, the tip has been made softer and, in addition, the excess traction of the first version has been corrected since, if it was not firmly positioned in the left coronary artery and it did not remain within the ostium, the catheter tended to recover its initial curve and could draw the guidewire out of its position in the coronary artery. In addition to the improvement in the catheter in this respect, it is recommended that it be left for 3 to 4 min with the guidewire introduced as far as possible into the interior prior to using it in the patient and, thus, straighten part of the initial curve.
Two studies have described its utility in interventional procedures involving the radial approach in complex lesions. Liang et al2 reported the simultaneous implantation of two stents using the kissing balloon technique and Mamas et al,3 in 16 cases, employed techniques such as the implantation of two stents in bifurcations, thrombectomy with devices that required conventional 7-Fr catheters, the use of Proxis® and RA with 1.25-mm, 1.5-mm and 1.75-mm burrs. The results of our work support the utilization of this catheter in RA and, moreover, describe its use with burrs of up to 2mm, thus demonstrating the possibility of increasing the range of the utilization of this technique via the radial approach.
Received 12 August 2010
Accepted 29 September 2010
Corresponding author: inigo.lozano@gmail.com