To the Editor:
Stents implanted into hard, calcified lesions do not always fully expand, even though they are inflated at very high pressure, and once the device has been released the problem is difficult to solve. The ablation of the stent and the calcified plaques protruding through the stent rings by means of high-speed rotational atherectomy reduces wall thickness, facilitating balloon dilation. This technique, which is not without potential risks, has been successfully employed in three patients.1,2
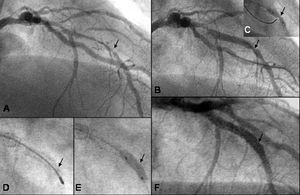
A 70-year-old hypertensive, hypercholesterolemic man was admitted to our hospital for acute coronary syndrome with ST segment depression in anterior leads. The results of physical examination, chest radiography, blood cell count and standard laboratory tests, including serial determinations of creatinine phosphokinase level and troponin T expression, were normal. In addition to the treatment he was receiving at the time of admission, consisting of atenolol, atorvastatin and aspirin, clopidogrel, and intravenous infusion of nitroglycerin was initiated and cardiac catheterization was performed. The left ventricle, which was hypertrophic and presented moderate hypokinesia of the apical region, preserved an ejection fraction of 63%. The bifurcation of the left main cononary artery presented a stenosis of 40% and subtotal occlusion of the ostium of the circumflex artery. This vessel, which was occluded distally, was being supplied via inadequate collateral circulation branching from the right coronary artery, which presented severe stenosis of the middle segment. All these lesions were successfully treated by means of stent placement. The left anterior descending coronary artery (Figure, A), possibly the culprit vessel, presented an extensive severe, calcified stenosis of the middle segment. After predilatation using a 2.5x25-mm Maverick balloon, a 2.75x24-mm Driver stent was implanted; however, a portion of the distal third did not expand completely, presenting a diabolo-like image (Figure, B). An attempt to post dilate using a 3.0x13-mm Powersail balloon inflated to a pressure of 25 atmospheres failed (Figure, C), and therefore rotational atherectomy using a 1.75-mm olive-shaped burr (Figure, D) was carried out. Afterwards, post dilatation resulted effective, and a 3.0x12-mm Taxus pharmacoactive stent was deployed into the previously implanted stent (Figure, E). The final angiographic result was excellent (Figure, F) and there were no adverse events. The postoperative course was satisfactory and the patient, when discharged from the hospital 48 hours later, was asymptomatic. At 5 months, coronary angiography revealed the absence of restenosis in the Taxus stent.

Figure. Angiographic sequence. The arrows indicate the location of the underexpanded ring in each image. A: anterior descending coronary artery prior to the interventional procedure. B: predilatation and implantation of a stent (2.75x24 mm), showing the underexpanded ring. C: unsuccessful postimplantation dilatation at 25 atmospheres. D: intra-stent rotablation with a 1.75-mm olive-shaped burr. F: repeated postimplantation dilatation followed by drug-eluting stent placement (3.0x12-mm Taxus). F: final satisfactory angiographic result.
The efficacy of rotational atherectomy in situations of incomplete expansion of stents implanted in severely calcified lesions has been demonstrated in three previously reported cases in which there were no problems associated with the erosion of the metal.1,2 The success may be attributed to the ablation of the stent rings and the calcium that protruded through them, resulting in the thinning of the wall. Although certain potential complications, such as the distal embolization of metal particles or late thrombosis, could develop, they did not occur in any of the four cases documented in the literature. Our case confirms the feasibility of this technique in special cases.