The correct answer is number 3: monomorphic ventricular tachycardia and atrial fibrillation. On analysis of the device, it was found that the atrial arrhythmia presented first at a high frequency (160 bpm) and this was followed by ventricular tachycardia (150 bpm), probably induced by the ventricular tachycardia response. External synchronized electric cardioversion was performed, and sinus rhythm was achieved with a biphasic 150J shock.
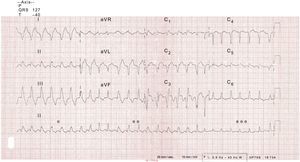
Ventricular tachycardia beats (*), beats with differing degrees of fusion (**), and narrow complex atrial fibrillation (***) can be observed in the rhythm strip (Figure).

Answer 2 is incorrect because atrial fibrillation with aberrant conduction would not have regular periods and there would be no fusion beats. Answer 4 is incorrect because pre-excited atrial fibrillation with a left lateral accessory pathway would sometimes be irregular and the QRS complex between V2 and V4 should be largely positive. Likewise, answer 1 is incorrect because polymorphic ventricular tachycardia would show a clear shift in the electrical axis at higher frequency.