Keywords
INTRODUCTION
The ever increasing consumption of cocaine over the last few years has made Spain one of the greatest consumers, together with the United States and the United Kingdom.1-3 According to the World Drug Report for 2009 published by the UN, 1.4% of the population of Western Europe between the ages of 15 and 64 and 3% of the population of Spain, consume cocaine.1 These percentages are greater in certain age groups, such as secondary school students, in whom cocaine consumption in Spain has quadrupled in the last 10 years.2,3
This alarming increase in cocaine consumption correlates with a corresponding increase in medical consultations. Therefore, in 2005, 75% of the consultations in the Emergency Service caused by illegal drug abuse in a tertiary hospital were due to intoxication by cocaine,4 and in these, chest pain was seen in 8%-16%,5 a fact that is little known and, frequently, undervalued.
The lack of available information on the management and prognosis of these patients,6-11 especially in Europe, and the existence of discrepant data on the incidence of acute myocardial infarction related to cocaine consumption12-19 make it necessary to perform specific studies. The aim of this study was to analyse the prevalence of cocaine consumption in patients who consult for non-traumatic chest pain in a general hospital, to study the clinical characteristics of the patients and to estimate the frequency of acute coronary syndromes in this population.
METHOD
All the patients, in consecutive order, who came in to the chest pain unit (CPU) of a university hospital during the course of the year were assessed. In all patients a standard questionnaire was used to register prospectively their clinical history; it included data on history of diseases, cardiovascular risk factors, previous treatments, characteristics of the pain, physical exam, ECG, blood analysis and treatment given. Specifically, a question on recent consumption of cocaine was included. In this manner we identified those patients who came in to consultation for chest pain who reported consumption of cocaine within the last 24 hours. According to medical criteria, on admittance to the Emergency Service the presence of the main metabolite of cocaine (benzoylecgonine) was assessed by qualitative enzyme immunoassay using the Dade (Behring®) reagent.
Patients
All patients were treated following the usual protocol for the CPU of our centre, the physical, functional, organisational and care characteristics of which have been described above.20
In all cases and after initial clinical assessment and the performance of the first ECG, the initial diagnosis was made of: acute coronary syndrome (ACS) with ST segment elevation (ACSSTE); ACS with no ST elevation (ACSNSTE); possible ACS; non-coronary pain. Group 1 patients were immediately assessed for reperfusion treatment; all group 2 patients were assessed by a cardiologist and appropriate treatment begun; patients in group 4 were discharged or referred to the emergency service to continue their diagnostic process. Patients with a possible ACS and normal ECG remained in the CPU until the observation period of at least 6 hours was complete, having undergone a minimum of 3 serial ECGs and 2 troponin I determinations separated by 6-8 hours. If they were troponin negative, an ECG with stress test was programmed with an imaging technique,21,22 and their admittance was subject to the decision of the cardiologist. After completing the CPU protocol, the patients received a final diagnosis of acute myocardial infarction with ST elevation (STEAMI), or acute myocardial infarction with no ST segment elevation (nonSTEAMI), unstable angina or non-coronary pain. Unstable angina was only diagnosed in those cases having chest pain suggestive of coronary origin and negative troponin, signs of spontaneous ischaemia on the ECG (ST descent, negative T waves) or induced ischaemia with a stress test, or coronary lesions ≥50% in patients with a history of infarction.
Statistical Analysis
The clinical characteristics and the evolution of the cocaine consuming patients were compared with those of non-consumers. To avoid bias in the comparison, and since only 4.5% of the consumer patients were over 54 years of age in comparison with 63% of the non-consumers, only patients under 55 years of age were included in this study.
The qualitative variables are expressed in percentages and were analysed using the chi square test or the Fischer test, accordingly. The quantitative variables are expressed as mean (SD) and the differences were analysed using the Student t test. With the aim of estimating relative risk of infarction associated with recent cocaine consumption, a binary logistical regression analysis was performed and the odds ratio (OR) associated with this variable was calculated, adjusted for coronary risk factor, cardiovascular history of the patients and previous treatment. For the statistical analysis the SPSS 15.0 program for Windows was used.
RESULTS
During the study period a total of 3363 patients consulted the Emergency Service for non-traumatic chest pain; of these 1240 (37%) were less than 55 years of age and formed the study group. Initially 41 patients were diagnosed with ACSSTE, 35 with ACSNSTE, 323 with pain of possible coronary origin, and 841 with non-coronary pain.
Prevalence of Recent Cocaine Consumption
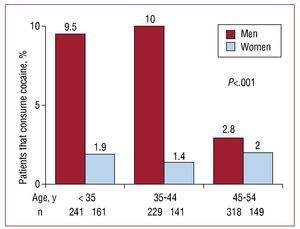
Fifty-three patients admitted having consumed cocaine recently, whereas 10 patients that denied it had a positive analysis for cocaine metabolites in urine. The prevalence of recent cocaine consumption was 5% (63 out of 1240), 7% (55 out of 789) in men and 1.8% (8 out of 451) in women (P<.001). Frequency of consumption in men varied with age, between 2.8% in patients between 45 to 55 years of age and 10% in those under 45 years of age (P<.001). In contrast, the frequency of cocaine consumption in women was similar for all age groups (Figure 1).

Figure 1. Distribution by age and sex of the prevalence of recent cocaine consumption in patients who came in to the emergency service due to acute chest pain. Significant differences can be seen between sexes and age groups. The mean frequency of cocaine consumption in men was 7% and it was inversely proportional to the age of the patients from 45 years upwards (P<.001), whereas in women it was 1.8% independent of age (P=.92)
Clinical Characteristics on Admittance
Previous cocaine consumption was seen in younger patients (35 [10] vs 39 [10] years; P=.002), and more frequently in men (87% vs 62%; P<.001) and smokers (59% vs 35%, P<.001) than non-consumers. No significant differences were seen in other coronary risk factors. Neither were differences seen between both groups as to previous cardiovascular history (13% vs 12%, P=.84), nor in treatment previous to admittance (Table).

The diagnostic orientation on admittance was based on anamnesis, physical exam, and ECG, and was significantly different in patients with and without recent consumption of cocaine, with a greater number of patients suspected of ACS with or without ST segment elevation in the cocaine consuming group (Table).
Final Diagnosis
Among cocaine consuming patients, the 7 patients with an initial diagnosis of ACSSTE were diagnosed with STEAMI, and of the 3 patients with ACSNSTE, 1 was diagnosed with nonSTEAMI and 2 with unstable angina. On the other hand, of the 13 patients with an initial diagnosis of chest pain of possible coronary origin, 2 were troponin positive and were diagnosed with nonSTEAMI; of the remaining 11 patients, 3 were admitted and unstable angina was ruled out, in 6 a diagnostic stress test was performed that ruled out ischaemia and 3 patients refused to carry out the stress test and requested voluntary discharge.
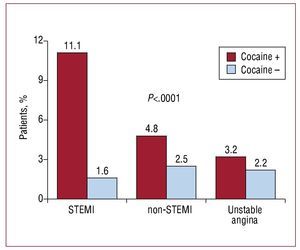
Globally and out of a total of 1240 patients studied and after complete assessment in the CPU, 26 patients (2.1%) were diagnosed with STEAMI, 32 (2.6%) with nonSTEAMI, and 28 (2.3%) with unstable angina. Myocardial infarction was diagnosed in 10 patients with cocaine consumption and 48 patients with no cocaine consumption (16% vs 4%; P<.001). This greater frequency of myocardial infarction was especially due to the number of cases with STEAMI, 7 (11.1%) versus 19 (1.6%) (P<.001) (Figure 2).

Figure 2. Differences in final diagnosis of each type of ACS according to previous cocaine consumption among patients that consulted due to chest pain. The patients who had recently consumed cocaine suffered a higher rate of infarction (17% vs 4%, P<.001) than patients who had not consumed cocaine, especially in cases with STEAMI.
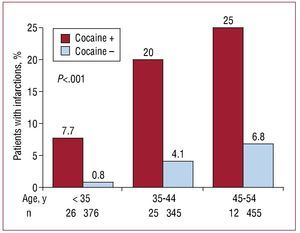
The absolute risk of infarction was directly proportional to age in both groups of patients (P<.001), whereas non-adjusted relative risk of infarction for cocaine consumers in relation to non-consumers was 4.4 (95% CI, 2.1-9.3; P<.001), with no significant difference seen in different age groups (Figure 3).

Figure 3. Frequency of acute myocardial infarction in each age group in patients who came in to the Emergency Service due to acute chest pain, according to whether they had consumed cocaine or not. The absolute risk of infarction was directly proportional to age in both groups of patients (P<.001). The non-adjusted relative risk of myocardial infarction with or without ST segment elevation was 4.4 (95% CI, 2.1-9.3; P<.001) times greater among cocaine consumers in relation to non-consumers, with no significant differences seen between different age groups.
In the multivariate analysis and after adjusting for coronary risk factors, cardiovascular history and previous treatment, the recent consumption of cocaine was associated with an odds ratio of infarction of 4.3 (95% CI, 2-9.4).
Clinical Management
During their stay in the CPU, all patients with infarction and previous consumption of cocaine were treated with aspirin, 60% with clopidogrel, 90% with heparin, 60% with beta-blockers, 90% with nitrates, 10% with calcium antagonists, and 50% with benzodiazepines.
Of the 7 patients with STEAMI, 6 underwent primary angioplasty and 1 patient thrombolysis followed by angioplasty. Coronary angiography was performed in the 3 patients with non STEAMI, 3-vessel disease was seen and treated by surgical revascularisation in 1 patient. The other 2 patients did not have significant lesions; in both cases an echocardiographic study showed the existence of regional anomalies during contraction with preserved ejection fraction. In summary: coronary angiography was performed in 10 patients, 2 had no significant lesions, 3 had 1-vessel disease, 4 had 2-vessel disease, and 1 had 3-vessel disease. Coronary spasm was not seen in any of the patients, and complicated lesions with thrombi were seen in 80% of the patients. A patient with a lower AMI and a history of percutaneous revascularisation with a stent in the LAD had a thrombotic occlusion of the stent and the right coronary artery.
DISCUSSION
We describe the prevalence, clinical characteristics and final diagnosis in a consecutive series of patients with chest pain associated with recent cocaine consumption in patients under 55 years of age that came in to the emergency service due to chest pain. The most significant results were the high rate of recent cocaine consumption in these patients, especially in men, and their quadrupled risk of presenting acute myocardial infarction.
Cocaine Consumption and Consultations Due to Chest Pain
The percentage of patients less than 55 years of age that consulted in the emergency service due to chest pain associated with cocaine consumption was 5%. Globally, in all patients of all ages, the frequency was 2%, a similar percentage to the 1.7% reported in a hospital in the United Kingdom11 and the 2.7% seen in the study Acute Cardiac Ischaemia-Time Insensitive Predictive Instrument (ACITIPI)15 in the USA, in concordance with the greater consumption of cocaine in the general population in these countries.1 Therefore, among patients under 45 years of age the frequency was similar (10% vs 12%).
It is important to highlight that in our study, 19% of the patients did not admit they had taken cocaine in spite of cocaine metabolites being detected in urine. Other studies have shown that between 30% and 50% of the patients with positive cocaine tests in urine do not admit consumption.10,23 Furthermore, in the only study in which a systematic study of urine was performed in all the patients who came in to the emergency service due to chest pain, it was seen that 17% of the patients tested positive.23 Therefore, these rates of prevalence are probably underestimated.
In our study the frequency of cocaine consumption was 4 times greater in men than in women, whereas in other studies the ratio of men to women was 2-3 times greater.15,18,23 On the other hand, we wish to highlight that the prevalence of cocaine consumption among men was markedly different according to age, reaching 10% among those less than 45 years of age, percentages which are similar to those seen in other large studies.15 In contrast, among women the frequency was 1.7% in all age groups.
Questions on Cocaine Consumption in the Emergency Service
The questions on drug consumption in the emergency services tend to be very variable, and, in any case, this factor has much lower values than the classical factors of coronary risk.8,9 Therefore, in 1 study only 31% of the patients seen in the emergency service for chest pain were asked if they had consumed cocaine, and this fact was only registered in the clinical history of 13% of the patients.8 In another recent study carried out in the United Kingdom,9 specific questions on cocaine consumption were only carried out with 3.7% of the patients. In contrast, one of the strong points of our study was the application of a standard questionnaire that ensured questions were asked on this factor and registered in the patients' clinical history.
Myocardial Infarction and Recent Cocaine Consumption
Of the patients who consulted due to chest pain after having consumed cocaine 17% suffered an infarction. This high incidence rate of infarction contrasts with what has been seen in other studies that found a wide variability between 1% and 16%.12-19 Differences in the type of population studied, in the consumption pattern or in the necrosis marker used may explain the greater incidence of infarction in our series. It must be pointed out that in 2 recent studies17,19 that used troponin as a marker of myocardial necrosis, myocardial infarction was diagnosed in 14% and 16% of the patients, respectively.
In our study, the patients with chest pain associated with cocaine consumption had a mean age of 35 years and few coronary risk factors. Nonetheless, they had a high incidence of myocardial infarction, especially with ST segment elevation. The risk of infarction adjusted by risk factors, cardiovascular history and previous treatment, was 4 times greater in patients with recent cocaine consumption than in the control group, independent of the age of the patients. This agrees with the data of other large studies that have reported that the risk of infarction in these patients is much greater and can be increased by a factor of 7 in patients less than 45 years of age.24 Furthermore, the probability of suffering an infarction in the hour following cocaine consumption is up to 24 times greater.25
Multiple mechanisms have been proposed as the cause of acute coronary syndrome due to cocaine consumption. Cocaine increases oxygen consumption by inducing tachycardia, arterial blood pressure elevation and increase in myocardial contractility,26 and induces coronary vasoconstriction,27 which could explain the reason approximately 20% of patients with infarction after cocaine consumption have normal coronary vessels.28,29 Furthermore, cocaine induces coronary thrombosis by stimulating platelet activation and aggregation30,31 and the generation of C reactive protein, fibrinogen, von Willebrand32 factor and inhibitor of plasminogen activator.33 The high prevalence of infarction and the thrombotic lesions seen in coronary angiography in the patients of our series illustrate this situation. Lastly, the high prevalence of smokers in this population, a factor which has been considered a coadjuvant for cardiovascular toxicity due to cocaine, must be noted.26
Management of Patients With Chest Pain Associated With Cocaine Consumption
The patients of our study that were diagnosed on admittance with possible ACS were managed according to the usual protocol used in the CPU, with repetition of ECG and troponin tests at 6-8 hours. This rapid observation strategy has been shown to be safe in patients that had consumed cocaine.16,18
In our study, no different management strategy was applied to patients with chest pain and previous cocaine consumption, probably due to the lack of specific studies in this patient population and the European Clinical Guidelines lack of attention to this factor.6,7 Recently the American Heart Association34 has published a document on the management of these patients. The most important recommendations are to use nitrates and calcium antagonists, as well as the performance of emergency coronary angiography if there is persistent ST segment elevation, or preferably when there are persistent electrical changes.
Limitations of the Study
The determination of cocaine metabolites in urine was performed according to clinical judgment, therefore there was probably an underestimation of the real prevalence of recent consumption of cocaine in our series. However, the use and compliance with a standardised clinical questionnaire ensured that specific questions on this factor were asked of all patients.
CONCLUSIONS
The consumption of cocaine is a growing social and medical problem, constituing 5% of the consultations in the emergency service for chest pain in patients under 55 years of age. In spite of the low prevalence of cardiovascular risk factors in these patients they have a 4 times greater risk of myocardial infarction.
To question patients concretely on this factor during chest pain assessment in the emergency service not only makes risk stratification for ACS possible, but also has important therapeutic implications. Therefore, the assessment of cocaine consumption must be included in future guides for care of patients with chest pain and ACS by the different scientific societies and must be generalised in daily clinical practice.
ABBREVIATIONS
ACS: acute coronary syndrome
CPU: chest pain unit
NSTEACS: non-ST-elevation acute coronary syndrome
NSTEMI: non-ST-elevation acute myocardial infarction
STEACS: ST-elevation acute coronary syndrome
STEMI: ST-elevation acute myocardial infarction
Full English text available from: www.revespcardiol.org
SEE EDITORIAL ON PAGES 1013-4
Study funded in part by FIS 07/0089.
Correspondence: Dr. X. Bosch.
Unidad Coronaria. Servicio de Cardiología. Hospital Clínic. Villarroel, 170. 08036. Barcelona. Spain
E-mail: xbosch@clinic.ub.es
Received February 2, 2010.
Accepted for publication April 28, 2010.